
When everyone is thinking alike, then somebody isn’t thinking. Gen. George Patton
If you’re the smartest person in the room, find another room. Michael Dell (Forbes magazine)
“As God has said, and I think he’s right…” Margaret Thatcher
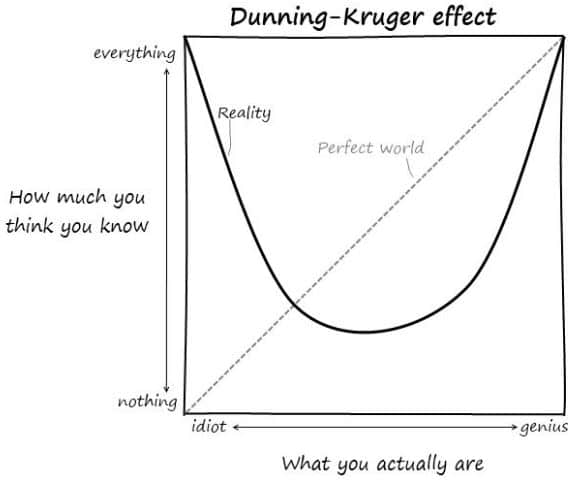
Dunning and Kruger were the first to systematically investigate unconscious incompetence and report their findings in the psychology literature. 1,2 Too bad for them, they will forever be remembered as discoverers of the Dunning-Kruger effect (DKE), a form of cognitive bias.
DKE is the defining characteristic of people who rate their own performance as high when, in fact, it is dismally low. Worse, Dunning-Kruger sufferers are doubly cursed because they lack the tools to evaluate their own performance and therefore cannot improve:
“The skills needed to produce logically sound arguments, for instance, are the same skills that are necessary to recognize when a logically sound argument has been made. Thus, if people lack the skills to produce correct answers, they are also cursed with an inability to know when their answers, or anyone else’s, are right or wrong. They cannot recognize their responses as mistaken, or other people’s responses as superior to their own.”
Just Another Cognitive Bias
In recent times all eyes and ears have been trained on the hearing health profession. There have been some seemingly illogical conclusions, or at least contradictions, reached by various stakeholders:
- Price as the main obstacle to hearing device uptake is a conclusion that will not go away, even though the data don’t support it as correct.
- Lack of access to hearing healthcare is another conclusion that will not die, notwithstanding evidence to the contrary.
- PSAPs are good. PSAPs are bad.
- OTC hearing aids are good. OTC hearing aids are bad.
- Patients will suffer. Consumers will benefit.
- Etc, etc.
Such conclusions lend themselves to cognitive biases, “anchoring,” where decisions (or votes) are made based on a single characteristic or first source of information, rather than a comprehensive weighting of data from all sources; or “confirmation,” where decisions are made only on the information that resonates with what we already believe. It’s human nature, otherwise psychology wouldn’t lump all such behaviors under the rubric of cognitive bias.
But are the concluders and deciders wrong just because they’re influenced by cognitive biases? Are they all DKE sufferers wreaking havoc on audiology and its acolytes just because they don’t know what they don’t know? Is an intervention called for?
Not unless we can convince ourselves that we are free of DKE and associated biases. This post explores the idea that we are just as likely to jump to conclusions and ignore what we don’t know as others.
Are You Talking to Me?
DKEs are, and remain, “blissfully unaware” of their shortcomings. All of us have seen and marveled at DKE sufferers, though naturally we blissfully don’t include ourselves among the victims.
Nailing others as DKE but not ourselves is part of yet another all-pervasive psychological phenomenon, the bias blind spot discussed in a prior post. We can’t help but subconsciously see and rate ourselves as better and less judgmental than most others. But, we remain blissfully unaware of our bias unless something forces it to our conscious attention and we have the opportunity to make ourselves aware (another psychological process, cognitive dissonance, may get in the way of of that).
Dunning-Kruger and bias blind spot do not measure intelligence, but they can measure discrepancies in performance and self-assessment of performance, as well as receptivity to feedback on both. Radiologists, for example, are smart and well-trained professionals with good reason to be confident in their diagnostic skills. Yet, published data shows that they “… perceive their performance to be better than it actually is and at least as good as their peers.”
Audiologists are smart people, by and large, but that does not immunize us against DKE. Bias blind spot to the contrary, we are not likely to be any better than radiologists when it comes to professional functionality. The following are two examples that come to mind.
DKE Example #1
In response to the OTC and PSAP debates and legislative efforts, the following wide-ranging comment hit the Hearing Economics desk:
The Brain’s plasticity is lost when the consumer buys a PSAP. That is the price paid to save money and avoid the use of an Audiologist. It’s that simple. The Audiologists who have failed to recognize that the ONLY third party way that one can ethically buy hearing aids is from a certified GPO like 95% of hospitals do here in USA. Audiologist can buy direct from the manufacturer but ALL third parties like Buying groups and Management groups especially those that private label and lock their AIDS are functioning unethically because the Audiologist does not know the margins and cost of services built into the invoice.
Opinions stated as facts are not evidence of critical thinking, but they do send up DKE red flags.
- There is no evidence that brain plasticity is lost when consumers purchase PSAPs, whether they wear them or not. In a controlled study of consumer choice, the probability seems low that consumers would trade brain function for PSAPs. But we could test that hypothesis.
- Accusations of unethical behavior are inflammatory and misguided: Business ethics need not be the same as professional ethics and professional ethics differ among professional groups as defined in different state licensure laws.
- Knowledge of suppliers’ internal costs has little or no bearing on running a business well or practicing professionally. Suppliers and audiologists are both tasked with running their businesses efficiently by controlling costs. Purchasing without evaluation from any source reflects poorly on their business judgement and will likely have an adverse effect on margins, carried over to retail sales price, creating a deadweight loss in economic parlance.
Misinformation, disinformation, inflammation, and indifference are DKE red flags which the market will not tolerate in the long run, or so Hearing Economics hopes.
DKE Example #2. A Rising Bank Account Raises All Egos
Pursuant to the last item in Example #1, consider private practice audiologists who are doing well financially in spite of their lack of business knowledge, accounting practices or due diligence, all of which may move them in the DKE column. Here’s the response of a successful audiologist to a quantification question posed by Hearing Economics:
Q: What is your percentage increase in hearing aid invoice costs over the last few years?
A: I’m not a “numbers gal.” I personally don’t keep track of how many hearing aids I sell in a week or a month. In X years, I have always focused my attention on how I’ve cared for my patients. Take care of them, and they will take care of you. I know that approach would drive the Type A personalities absolutely nuts!!!!!!!!!
The answer has nothing to do with the question. Cost of Goods (COG) is largely independent of how many one sells at what price or how one treats patients. Some people get lucky and find that a winning personality plus good location afford them a positive bottom line, leading them to believe that they are successful because of personal attributes, independent of good business measures.
This is critical thinking failure at its best. It’s nonsense to cover up a lackadaisical approach to running a practice by claiming success because of favorable circumstances or by using a bunch of exclamation points. Equally nonsensical is the use of the “point at someone else” trick to divert attention away from one’s lax behavior by painting other audiologists who count as “numbers people” of Type A persuasion. By implication, Audiologists-Who-Count are bad because they are tallying instead of focusing on their patients.
Why Are These Problematic for Our Profession?
Example 1 seems self-explanatory. We do ourselves and our patients a disservice by spreading false information or standing in our bias blind spot to point the finger at other providers or entities for sub-standard professional behaviors.
Example 2 requires a bit of explanation to support the claims that DKE Audiologists are bad for the economy and poor role models for newly minted Audiologists.
- Audiologists who won’t count are bad for the economy. They are not watching their COG and adjusting their Prices to reflect competitive changes in the Goods Market. They’re acting like Price Makers because they can, which we all know from reading Hearing Economics creates unsustainable market inefficiencies, meaning that eventually those pseudo Price Makers no longer can. The 2016 PCAST recommendations and 2017 OTC legislation are reactions to market inefficiencies of this type.
- Audiologists who won’t count are bad for their practices. Eventually, their luck runs out which creates a ripple effect that harms employees and patients. Enter Costco and more business-savvy audiologists who can care for clients/patients and count. Their competencies enable data-driven Pricing which offers more Marginal Utility (Willingness to Pay) to consumers than a winning personality. The DKEs never know what hit them. They blame the Big Box, the Economy, the Present Administration, the manufacturers, fickle patients, PSAPs — anybody but themselves.
- DKE Audiologists are poor role models. Perhaps more than successful non-DKEs, they may feel a compelling need to spread their success by inviting 4th year externs to work and learn in their practices. This makes sense — students naturally want to go to successful practices to learn how to be successful and many owners who see themselves as successful-by-dint-of personality also like to have cheap or free labor. They may not count margins but they definitely count dollars (see bias blind spot post). In such environments, it seems likely that DKE mentoring can (mis)lead students into DKE territory from which they may never return. Medical research supports this probability. The externship itself produces a newly-minted generation of DKE Audiologists.
The DKE Within
We have met the enemy and they are . . . bloggers? Maureen Dowd, NYTimes columnist
Off the cuff comments and and outsiders’ perspectives on private practice activities are low hanging fruit for bloggers in search of DKE symptoms. By the same measure, writing about DKE, much less blogging on a weekly basis, are sure signs that one suffers from DKE of one sort or another, otherwise we’d have run out of things to write about long ago. Thank goodness for our bias blind spots.
It is vexing to understand that none of us escape DKE in at least some aspect of our lives. But that understanding is the first step toward recovery in whatever realm we falter. The good news about DKE is that it can be altered by a teachable moment, as in when the blog you just wrote is nonsensical, your practice collapses, your favorite patient leaves you for Costco, your best friend quits talking to you, or somebody or something demonstrates unequivocally that your performance is below that of others.
We can all benefit on a daily basis by staying alert for teachable moments. Teaching by non-DKE instructors and professionals in graduate programs and continuing education forums is critical for our profession. Likewise, ferreting out DKE instructors and practitioners is critical to survival of the profession, as is striving for unbiased, fact-based discussion and research among academics, those in industry, practitioners and consumers. A recent discussion of DKE in Emergency Medicine settings (Shaw, 2016) emphasizes immediate feedback, daily/weekly review, continuing education, and humility as important tools for clinicians to combat DKE performance and judgement errors
Many audiologists work hard at such endeavors and we all benefit from their efforts. Critical thinking is a learned skill that can be applied full time for the benefit of clinicians and their patients. Wouldn’t it be great if it were a graduation requirement for doctoral students and a condition of employment and licensure? Out in the field, Best Practices and other means of measurement are efforts to teach and improve our profession through the judicious use of supportable research and clinical data. There are many continuing education opportunities within and outside our field. There are many experienced practitioners to learn from.
In the meantime, please count well and often for the benefit of your patients, your practices, our profession, and the economy. And try not to blame PSAPs or OTCs for plummeting profits or brain malfunctions, including DKE.
References
1Kruger, Justin. (1999) Unskilled and unaware of it: How difficulties in recognizing one. Journal of Personality and Social Psychology, 77(6), 1121-1134. DOI: 10.1037/0022-3514.77.6.1121
2 Dunning, D. (2003-06) Why people fail to recognize their own incompetence. Current Directions in Psychological Science, 22(3), 77-87. DOI: 10.1111/1467-8721.01235




This is by far the best article I have ever read on the topic of general dysfunction in the industry and profession. It explains so much about where we are today and how we got here (although it does not delve into the complicity of manufacturers that have taken full advantage of these tendencies). You have increased my own self-awareness and given me tools to help other DKE sufferers battle this insidious affliction. Thank you, thank you, thank you!
I love this article. DKE affects every aspect of our lives.