
Dr. Richard Price has probably done more than any one researcher to delineate the potentially damaging aspects of impulse noise on our auditory system. He did most of his work in the 1980s and 1990s at the U.S. Army Research Laboratory, but had continued to publish well after his military incarnation. Of course the military is concerned about minimizing the chances of their soldiers getting a hearing loss from loud gun blasts, and in many cases, they are holding these noise-generating devices quite close to their ears.

Holding a noise generator by the right ear. Courtesy of www.YouTube.com
We don’t have any good models on the effects of impulse noise on hearing loss. Our “traditional” models based on increasing damage over exposures to 85 dBA and greater are relatively good but really only apply into the 112-115 dBA range. For sounds with exposure levels above that such as 140 dBA from a gun blast or a smashing together of two blocks of wood, we really don’t have a good sense of what we should do. Certainly, in these extreme cases, more is better…. We want to attenuate or lessen the sound as much as is possible but even then we are not sure about the potential long-term damage.
One of the areas of difficulty is that we are not actually sure what ultimately gets through to the cochlea of the listener. If we measure the sound level to be on the order of 140 dBA a meter from the listener’s ear, there can be some amplification in the 2700 Hz region (the G near the top note on the piano keyboard) caused by the listener’s outer ear canal resonance, and then some attenuation as the sound is transduced through the eardrum and middle ear structures before it even reaches the cochlea in the inner ear.
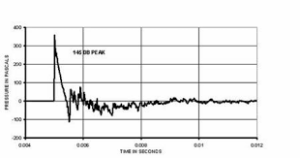
Impulse noise temporal response. Courtesy of www.arl.army.mil
We know that sound of any type is transduced through the middle ear to the inner ear optimally when the middle ear pressure is equal to the atmospheric pressure. After all, that is why children with ear infections and “negative middle ear pressure” have a (temporary) conductive hearing loss. The same would be true of any other sound, including impulse noise or music.
If the pressure wave of the impulse sound is either net positive or net negative relative to our atmospheric pressure then the impulse waveform will not be optimally transduced through the middle ear into the cochlea. But if the pressure wave passes through atmospheric pressure (0 mmH2O admittance equivalent) en route to the cochlea then this sound can be optimally transduced with a greater impact on the structures and function of the cochlea.

Courtesy of www.Arnsoldsofficefurniture.com
Therefore given two identical (peak) sound level impulse wave forms, one may be quite damaging (transduced at atmospheric pressure) and the other, less so (either net positive or net negative relative to atmospheric pressure).
Each impulse blast needs to have a temporal analysis performed in addition to its (peak) sound level. Two wooden blocks being hit together where the pressure wave is completely net positive would be less damaging than a gun blast of the same sound level and duration, where the pressure wave passes through atmospheric pressure.
Short of listing all of Dr. Price’s publications, just Google “Dr. Richard Price” and “Impulse noise” and a list (mostly in the Journal of the Acoustical Society of America) will come up. (And if you are not a member of the Acoustical Society of America, dollar for dollar, it is probably one of the best organizations to join).
Newer names to watch in this field are many, but if you like to Google, watch out for some of the great publications of “Dr. Colleen Le Prell” at the University of Texas- Dallas. And Colleen did not pay me anything to say this!





Hi ,A very personally interesting blog, I suffered severe sound exposure playing drums in a rock band for 50 years but was a sudden exposure 10 years ago, tinnitus ensued causing and continues to cause much grief, sleep, depression etc. My widex hearing aids need replacing I enjoyed the sound but didn’t do much for the T. I am trying Phonak B90 whilst louder and do a little more for the tinnitus they are rubbish for music, the highs and deep lows not good, for me the music is important as the T only allows me 1 week in 4 where I able to listen to music, the tinnitus distorts otherwise. Any help on choice of hearing aids I would take on board, incidentally the tinnitus tone is at 5250 hz about, had lots of expert treatment non improved it. neuromodulation reset, in my opinion, made it worse. Thanks for any help John Martin