
Yes, I am paraphrasing Jay Z to discuss effective treatment of Benign Paroxysmal Positional Vertigo – or BPPV for short. It is difficult now to imagine that when I first started practicing in the early 80s, canalith repositioning (CRP) techniques for BPPV did not exist.
My first exposure came when a personal friend came to my office with complaints of recurrent vertigo. She was an educated, athletic, affluent person, and the episodes were really impacting her life. I didn’t really know what to do for her, so I sent her to Johns Hopkins (about six hours away). She came back the next week having been immediately “cured.”
I was so curious about this magic treatment that it changed the course of my career.
A Brief History of Canalith Repositioning (CRP) for BPPV
Practitioners beginning their career after 1990 might enjoy a quick review of the road to repositioning. Brand-Daroff developed exercises based on the idea of habituating the response to repeated provocation. When patients started getting better in a couple of days, they knew they were on to something, and suspected “dispersion of otolithic debris from the cupula.”
I mention this because the head movements in the B-D exercises are not particularly effective at repositioning otoconia from the canal to the vestibule. They were never intended to do this. Then a couple of French researchers (most notably Alain Semont) modified the B-D exercises into a single treatment procedure and published impressive results of rapid symptom resolution. John Epley developed the less strenuous, and now famous, Epley maneuver, and introduced it to the United States.
After my friend came back cured from Johns Hopkins, I booked a flight to Dr. Epley’s next course. Dr. Epley’s path to acceptance and recognition of his maneuver was not an easy one. I made a point to sit with him at lunch at the course in Denver. He was aware, but unfazed by the critics. He knew he was right. I faced a small sample of that same skepticism and criticism when I started performing CRP in the early nineties.
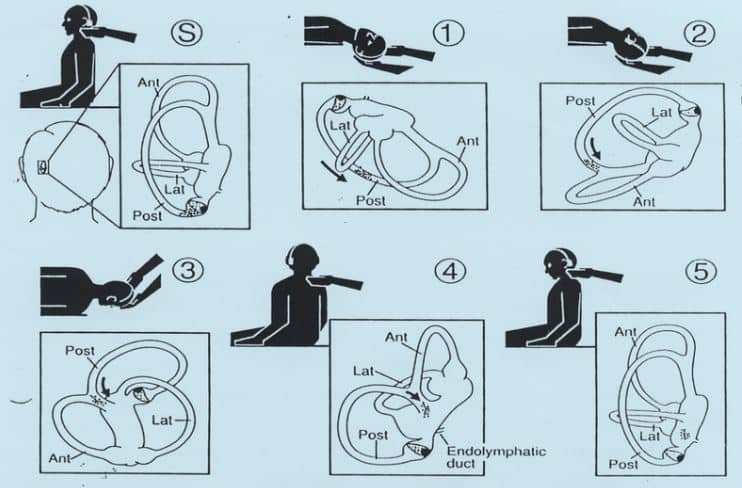
The Epley maneuver for treating BPPV. Otolaryngology — Head and Neck Surgery, 107(3), Epley JM, The canalith repositioning procedure: for treatment of benign paroxysmal positional vertigo, 399–404, Copyright Elsevier 1992
We now have many variations of canalith repositioning. In addition to the Epley and Semont, we now have the Zuma, Gans, Appiani, Casani, Gufoni, Asperella and DiCaprio (just kidding on that last one).
We have the home Epley, the Somersault, the BBQ roll and Brandt-Daroff for home treatment. All are based on the premise of using gravity to move offending otoconia out of the affected canal and back into the vestibule.
Is there a role for Meclizine in treating BPPV?
Despite consistent, continued evidence of the effectiveness of CRP, there still seems to be a knee jerk reaction in the medical community to prescribe meclizine (Antivert) for all complaints of vertigo.
The Clinical Practice Guideline for BPPV (see below) recommends against the use of meclizine for treating BPPV. In the discussions during the development of the original guideline published in 2008, we felt that treating meclizine as a viable treatment option might prevent patients from getting simple, safe and effective repositioning treatment.
Meclizine should not be a first line treatment, but can play a useful role in managing nausea until and during CRP treatments. Many patients are not aware that meclizine does not treat the BPPV, just the nausea that accompanies it.
“MEDICAL THERAPY: Clinicians should not routinely treat BPPV with vestibular suppressant medications such as antihistamines and/or benzodiazepines. Recommendation against routine medication based on observational studies and a preponderance of benefit over harm.”
–Statement from 2017 BPPV CPG
Dr. Epley passed away recently. As a profession, we owe him a lot. Because symptom resolution is most often so immediate with canalith repositioning procedures, BPPV has received a lot of attention in the press over the years.
I believe this media visibility has brought many patients, not just BPPV patients, in for assessment and more effective treatment of a variety of vestibular disorders.


