
What are they?
This week’s post is brought to you by my current doctoral student, Brady Workman. Brady is working towards his degree at East Tennessee State University, known for a strong vestibular program. He is teaching me a few things about VEMPs.
Here’s Brady:
Vestibular evoked myogenic potentials (VEMPs) are measurements originating from the otolith organs of the vestibular system (saccule & utricle). VEMPs are a unique subtest in evaluation of the dizzy patient because most conventional means of vestibular evaluation rely on the measurement of horizontal semicircular canal function. The otolith organs are the “front to back”, “side to side” and “up and down” motion sensors of the inner ear, whereas the semicircular canals sense head turns. VEMPs may be elicited by any stimuli that causes vibration/stimulation of the otolith organs, but air conducted stimuli tend to be the most frequently used clinically.
The otolith organs have nerve projections to both the eyes and neck muscles, which is where we are able to record VEMPs. By evaluating the otolith organs, one is able to develop a more comprehensive understanding of one’s vestibular function; thus VEMPs are complimentary to other, more traditional means of vestibular assessment, such as electronystagmography and/or rotary chair. VEMPs are capable of being recorded from several different muscles. For simplicity’s sake and clinical relevance, we will focus on the two most popular VEMPs, the Cervical VEMP (cVEMP) and the Ocular VEMP (oVEMP).
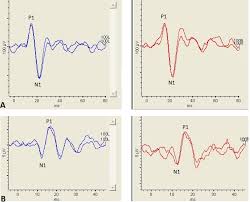
The cVEMP is primarily a measure of saccular function and is recorded on the sternocleidomastoid muscle of the neck. Bilateral recordings can be used when obtaining a cVEMP, but the main cVEMP response will be recorded from the sternocleidomastoid muscle of the ear that is stimulated. Due to the cVEMP response being reliant on the amount of underlying muscle activity, it is recommended that the clinician monitor muscle activity during cVEMP measurments. The cVEMP is characterized by an initial positive peak around 13 ms and a negative peak around 23 ms. Since the discovery of cVEMPs they have gained popularity as a clinical means for the evaluation of the saccule and inferior branch of the vestibular nerve.
Detailed recording parameters for measuring cVEMPs can be obtained from the “International guidelines for the clinical application of cervical evoked myogenic potentials: an expert consensus report”.
VEMPs have also been recorded from the eye muscles and are deemed oVEMPs (o for Ocular). The oVEMP is a more recent measure of vestibular function, and as such may be less utilized than the cVEMP. The oVEMP is primarily a measure of utricle function and can be recorded underneath the eye opposite the ear stimulated. The oVEMP is much smaller in amplitude than the cVEMP and has an initial negative peak around 10 ms and a positive peak around 15 ms. Although the oVEMP is of more recent discovery it has been shown as an effective clinical means of evaluating the utricle and superior branch of the vestibular nerve. More detailed recording parameters for oVEMP testing can be found here and here.
VEMP amplitudes are the most frequently utilized aspect of the response with responses from both ears compared to one another, utilizing what is known as an asymmetry ratio. By comparing the otolith function between ears the clinician is able to determine if the otolith organs are functioning properly and evenly between ears. Symmetrical functioning of the otolith organs between ears is necessary for proper sensation of movement and for balance maintenance. Overall, VEMPs are useful measures of otolith function that are complimentary to more traditional means of vestibular evaluation.




