

Holistic Audiologic Care: Echoing the Work of Arthur Boothroyd
Arthur Boothroyd, PhD
Nearly twenty years ago, Arthur Boothroyd authored an influential paper, published in Trends in Hearing, titled “Adult Aural Rehabilitation: What Is It and Does It Work?” While the concept of holistic care was not a new invention, Boothroyd’s work was pivotal because it effectively integrated decades of foundational perspectives on the importance of aural rehab from notable figures like Raymond Carhart, Patricia Kricos, and Mark Ross.
Boothroyd proposed a multidimensional model for hearing care, drawing on updated World Health Organization (WHO) terminology regarding how hearing loss impacts function, activity, and quality of life. He argued that comprehensive care must holistically integrate four key pillars: instruction, counseling, sensory management, and perceptual training.
Each of these elements is vital to the effective treatment of individuals experiencing hearing loss. They are summarized in Table 1.
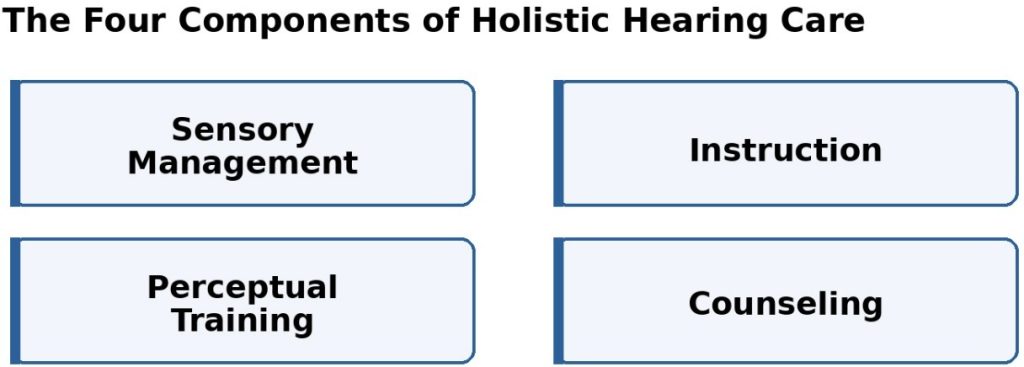
Table 1. According to Boothroyd (2007), the four components of holistic hearing care.
Each of these four components can be described as follows:
- Sensory management – selecting and fitting hearing aids or cochlear implants to enhance or restore audibility
- Instruction – providing education and guidance to increase the probability of a favorable outcome from hearing aids and other intervention strategies
- Counseling – providing personal adjustment and psychosocial guidance related to hearing loss and recommended treatment strategies to target issues related to participation and quality of life
- Perceptual training – auditory/cognitive training exercises that enhance listening skills needed for everyday communication
Modernizing Holistic Care with New Research and Technology
I have chosen to consolidate instruction and counseling into a single category for simplicity, as their objectives often overlap. This results in a “3-legged stool” model for holistic care, shown in Figure 1. This metaphor is particularly fitting because, much like a stool, the stability of a patient’s progress is compromised if any one of these three fundamental pillars is absent.
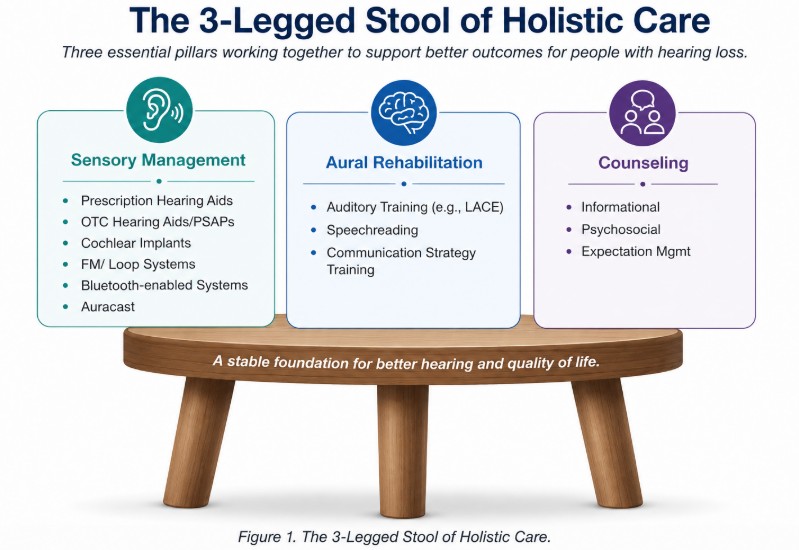
Ferguson et al. (2019) published an update to Boothroyd’s article, which strengthens the foundation of the “3-legged stool” model of holistic care. By leveraging updated research, they revisited the four original pillars to demonstrate how current, modernized tools for each component lead to better outcomes for patients. Their insightful analysis argued that the integration of smartphone applications and telecare can transition these core pillars—which form the three essential legs of the stool—toward a more autonomous and interactive patient experience.
In the years following their 2019 publication, AI has emerged as perhaps an even more significant catalyst for change in the clinical delivery of holistic care.
This outlook bridged the gap between Boothroyd’s foundational concepts and what’s possible due to modern technology, reinforcing the idea that stability in patient progress requires all three fundamental legs to be effective and present. Today, there is no reason a hearing care professional cannot offer something interesting, engaging and effective to help-seeking individuals that looks something like what is shown in Table 2.
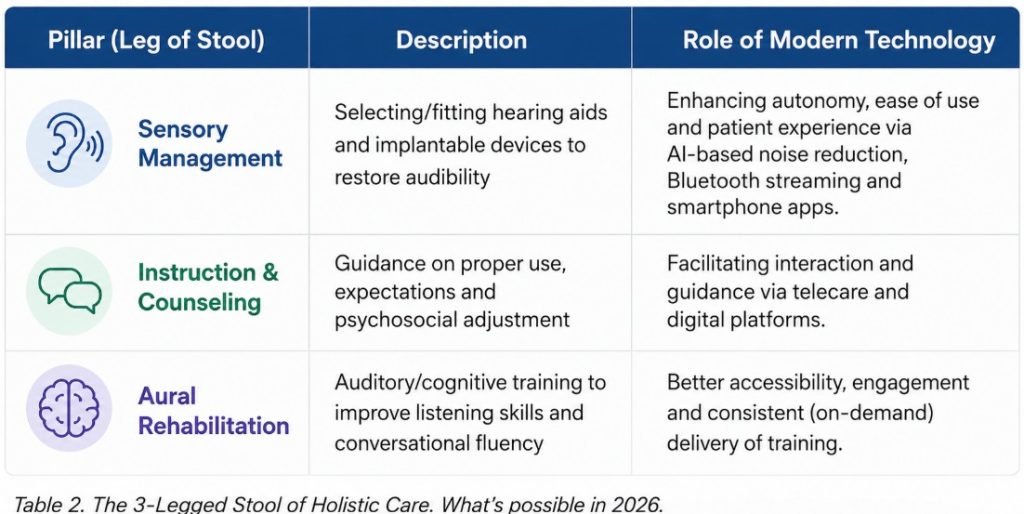
In the current clinical landscape, the three core elements of the “3-legged stool” model—sensory management, combined instruction and counseling, and aural rehabilitation—are no longer optional; they are fundamental to holistic hearing loss treatment. As noted by Henshaw et al. (2025), the evidence supporting auditory training—often the most overlooked component—is both extensive and expanding quickly.
These three legs are now the “table stakes” required to compete in a competitive hearing care market, but far too many in the profession still treat the aural rehab leg as a risky venture with uncertain returns. This must change. Hearing care professionals must step up as champions of true holistic care and commit to consistently ensuring all three legs of the stool are fully implemented in every single patient intervention. The evolution of audiology and the needs of our patients demand nothing less.
….And His Head in the Clouds
The Disconnect Between the Audiogram and Self-Reported Problems: More People Than We Think?
In early May, the Apple Hearing Study, conducted in collaboration with the University of Michigan, released key insights detailing a disconnect between normal audiograms and a person’s actual perception of a communication problem. They also found a direct link between hearing loss and reduced mobility, but that should not be a surprise—older people get hearing loss and walk slower for obvious reasons!
I think this is the most interesting finding for clinicians: Among nearly 85,000 participants who tested within the “normal” hearing range (4PTA < 25 dB), 16% rated their own hearing as fair or poor. These participants reported real-world difficulties with concentration and understanding speech when background noise was present.
To be more specific, many of the study participants who were classified as having normal audiograms had self-reported difficulties with concentration when listening to someone and when understanding others with background speakers. More than 7% of these participants rated the difficulty score larger than or equal to 8 (1 = not hard at all, 10 = very hard).
All told, this finding reminds us there are large swaths of individuals out there who might seek the help of a hearing care professional, present with vivid, undeniable problems related to an inability to communicate in important social and workplace settings, only to be told that “your hearing is normal.”
Ultimately, these results highlight a significant population of people who, despite seeking professional help for clear communication difficulties in social or professional environments, are dismissed with the claim that their hearing is “normal.” This raises a critical question: why is there not a universal standard to at least perform speech-in-noise testing? Furthermore, for patients motivated to resolve these issues, why aren’t interventions like low-gain hearing aids or self-directed auditory training more routinely provided?
Brian Taylor is a contributing editor to HHTM. He is also the VP of Clinical Research and Professional Relations for Neurotone. Opinions expressed here are his own. He can be contacted at [email protected].




