

Hearing Economics is pleased to welcome back the Guest Contributors from Ear Machine for Part 2 of Smartphone Control Apps.
Dianne spent 20 years at the University of Minnesota, teaching and doing research on hearing aids. She was director of advanced research at a major hearing aid manufacturer, and for the past 10 years has worked as a consultant to the hearing industry.
Andy is a hearing scientist and entrepreneur. He is an experienced researcher and developer of audio interfaces, especially for mobile and web.
Kevin is an Audiology Ph.D. who was head of clinical products and strategy at a major cochlear implant manufacturer. He’s an experienced researcher who is also an expert in distribution channels.
In our previous post, we made what we hope is a persuasive argument that hearing health professionals and consumers should insist that any smartphone hearing aid control app they use must be the product of substantial scientific research, and be usable with all hearing aids. In this post we review the scientific work of this type that we are aware of.
Who is doing large-scale scientific development work for control apps?
At present there are only two companies, to our knowledge, that are engaged in this type of scientific work. The first is Two-pi, a European company that is working with the Amsterdam Medical Center to develop and test a self-fitting and adjustment app based on a patented interactive audiovisual method for presentation of test sounds that are streamed to the hearing aid. Field trials are ongoing.

Ear Machine Controllers
The second is our company — Ear Machine. In our approach the user interface consists of two very simple-looking wheels that, when manipulated by the user, adjust all compression parameters in any WDRC hearing aid, smoothly in real time according to a hearing science-based algorithm, in any sound environment. If you’d like to try out the controllers, we recently released a free demonstration app for iOS devices. Our proprietary controllers are meant as universal applications to any (wireless) hearing instrument, just as NAL{{1}}[[1]] Byrne, D, Dillon, H., Ching, T, Katsch, R., and Keidser, G . (2001). NAL-NL1 procedure for fitting nonlinear hearing aids: Characteristics and comparisons with other procedures. J. American Academy of Audiology 12: 37-51. [[1]],{{2}}[[2]]Keidser, G., Dillon, H., Carter,L., and O’Brien, A. (2012). NAL-NL2 empirical adjustments. Trends in Amplification 16: 211-23.[[2]] or DSL{{3}}[[3]]Seewald, R., Moodie, S., Scollie, S., and Bagatto, M. (2005). The DSL method for pediatric hearing instrument fitting: Historical perspective and current issues. Trends in Amplification 9: 145-57.[[3]],{{4}}[[4]]Polonenko, M., Scollie, S., Moodie, S., Seewald, R., Laurnagaray, D., Shantz, J, and Richards, A. (2010). Fit to targets, preferred listening levels, and self-reported outcomes for the DSL v5.0 hearing aid prescription for adults. Int. J Audiol 49: 550-60.[[4]] methods can be used with any hearing aid.
Ear Machine Research: We have been awarded funding from NIDCD to do large-scale field studies, in partnership with Northwestern University, on the efficacy of the Ear Machine controllers. The University of Minnesota has been awarded another NIDCD grant to use our controllers to answer scientific questions about how people prefer hearing aids to be set in different noise environments. We would be delighted to hear from other interested research partners.
What Have We Found Out So Far?
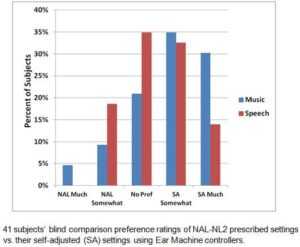
In Phase 1 of our research, subjects listen to pre-recorded speech-in-noise and music passages, and use the Ear Machine controllers, running on an iPod Touch simulating a 9-channel WDRC hearing aid, to adjust for maximum intelligibility and quality.
Preliminary data from our first 41 subjects (see Figure), ranging in age from 27 to 94, and in hearing impairment from mild to severe, show that after some initial practice, most subjects learn to make each adjustment in about 10 seconds, and that they:
- Make reliable adjustments (average test-retest < 4 dB);
- Select gain on average about -5 dB re: NAL prescribed gain (just as the subjects of Keidser et al.{{5}}[[5]]Keidser, G, O’Brien, A, Carter, L, McLelland, M, Yeend, I. (2008). Variation in preferred gain with experience for hearing-aid users. Int. J. Audiol 47: 621-635.[[5]] preferred gain about -5 dB re: NAL);
- Select gain close to NAL whether or not they start from settings appropriate for their hearing loss; and
- Like their self-adjusted settings as well or better than those prescribed by NAL, especially for music.
What’s Next?
After completion and NIDCD approval of Phase 1 of our research, we will begin field testing 100 subjects wearing wireless hearing aids controlled by Ear Machine controllers. That work will allow us to address questions related to how people set their hearing aids in their own environments, and how to determine what users are the best candidates for self-adjustment-enabled devices.
Whatever the research done by Ear Machine and others ultimately shows, professionals and consumers can expect several benefits from smartphone control technology:
For Hearing Health Professionals there will be new ways to differentiate their service models:
- In-office post-fit adjustment. Everybody has a story about the patient (usually an engineer or musician) who is never satisfied with how his/her hearing aids sound. Imagine being able to simply pass control to the patient in the office.
- In-the-field post-fit adjustment. One of the hardest things to get right in a hearing aid fitting is adjusting the aids to address the patient’s complaints about experiences in the real world. It is likely that research will show that at least some patients will be fully capable of using a self-adjustment app in the field. Expect to minimize return visits and maximize satisfaction.
- If research shows that some users can simply fit their own hearing aids from the get-go, after an initial audiological and otoscopic exam to establish candidacy, then this opens the door to offering a lower level of service to those patients, at correspondingly lower cost.
Consumers can expect to be able to use their smartphones to make their hearing aids sound better both in the clinic and, if supported by research results, in any other environment. There are many consumers who have known all along that they are fully capable of taking more control over their hearing aids, and for them, enhanced control of their sound environment will be a very welcome advancement in hearing technology.



