The 2014 updated list of research findings on the effects of caffeine and coffee on our health is here, with new findings highlighted in red. Even though the “benefits” column far outweighs the “risks” column these days, not everyone is on board when it comes to endorsing coffee/caffeine as a health supplement. But the barriers keep getting knocked down as Hearing Economics winds up its annual two-week celebration honoring International Coffee Day.
Tinnitus Drives You to Drink but Coffee Drives Out Tinnitus
The assumption that caffeine induces tinnitus is deeply ingrained in our Audiological psyches, history-taking, and patient counseling, despite a dearth of evidence to back it up. Now comes epidemiological research data saying that coffee lowers the risk of tinnitus, at least in women of a certain age. In the Nurses Health Study II (NHSII), coffee consumption and reports of tinnitus were tracked for 14 years for 65,085 women who were 30-44 when NHSII began.
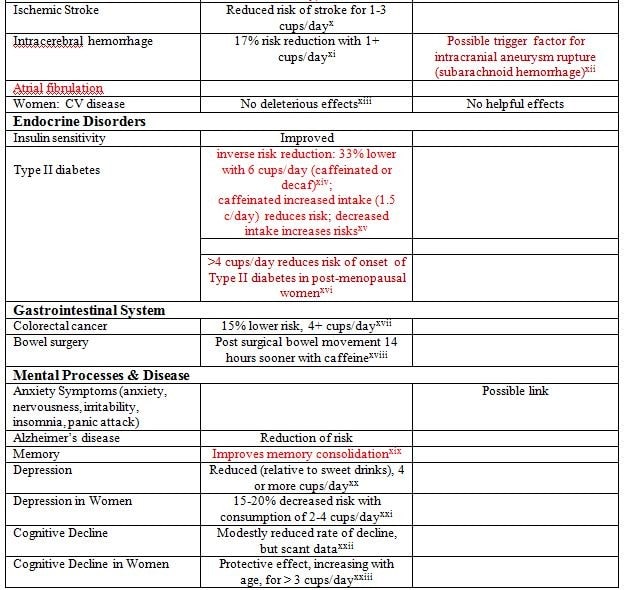
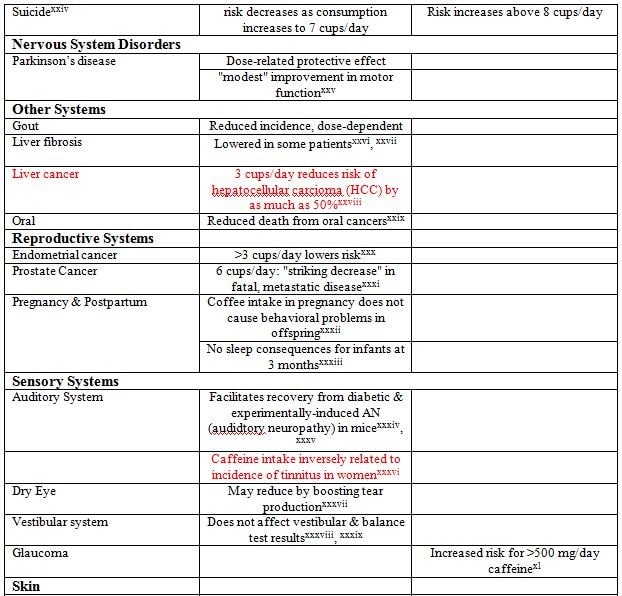
Much to Audiologists’ surprise, the study found that women who drank more coffee reported less tinnitus in a systematic way: caffeine intake was significantly, inversely associated with incidence of tinnitus. The risk of tinnitus was 15% lower for women who drank 3 to 4 cups/day and 21% lower for those who drank more, compared to women who drank less than a cup/day. {{1}}[[1]]Glicksman JT, et al. A prospective study of caffeine intake and risk of incident tinnitus. Am J Med, 127(8), 3/6/2014.[[1]]
Got Research?
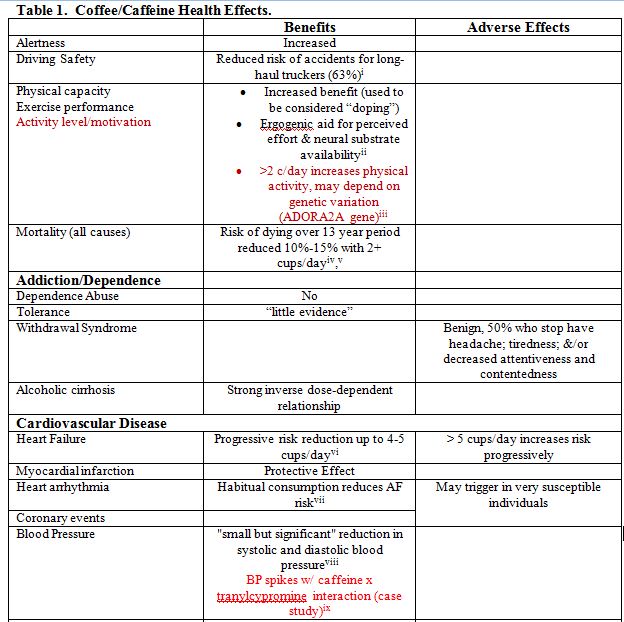
The table below contains study after study showing coffee significantly affecting one or another bodily system, which begs two questions about research in general and this table in particular.
Q1: How many of the significant findings in the table are statistical flukes?
A1: More than you’d think. Most studies use a P value, usually .05, as a statistical line in the sand to distinguish “significant” findings ([p<.05) from normal sampling variation (p ≥ .05). But these are probabilities, meaning that your finding has a 5% chance of being a chance event. Worse, if you replicate your study to ensure you’ve really got something, you have a 9.75% chance that one of your significant findings is a random event, another way of saying it’s wrong. Even worse is what the popular media has dubbed science’s “replication crisis” in which one-time significant findings are accepted as the real deal without repeating to check for chance.
Even if there is no real effect in your data, you have over a 40% chance of finding a fake effect if you do the analysis 10 times. Apparently, some researchers have caught on to that and keep at it till they get the (random) result that yields (spurious) significance. So says Christopher Labos, MD, in a delightful article that tells you why you need to take the table below with a grain of salt and not put all your money into Starbucks stock.{{2}}[[2]]Dr. Labos’s article is at Medscape, which is a free site, but requires registration for access. It’s worth registering to get his article and many other daily top stories.[[2]]
Q2: What does statistical significance imply about clinical significance?
A2: Nothing if the study is biased. Dr. Labos explains a variety of bias types that render findings meaningless, including selection bias, which he illustrates perfectly with coffee:
a 1981 NEJM study showed an association between coffee consumption and pancreatic cancer. The selection bias occurred when the controls were recruited for the study. The control group had a high incidence of peptic ulcer disease, and so as not to worsen their symptoms, they drank little coffee. Thus, the association between coffee and cancer was artificially created because the control group was fundamentally different from the general population in terms of their coffee consumption. When the study was repeated with proper controls, no effect was seen.
Are You Feeling Lucky?
Dr. Labos makes one more helpful coffee-driven statistical point about pitfalls of risk descriptions, such as in the NHSII-tinnitus study above. His main point is that non-case studies need to use relative risk ratios (RRR) and not odds ratios because the latter overstate risk and scare people. Audiologists, don’t worry — the tinnitus study used hazard ratios, which are a special form of relative risk ratio that works to minimize selection bias.
His secondary point is that relative risks are ratios that say nothing about absolute risks, which are rarely reported in studies even though they are the ones that are most useful in making health decisions. He uses another excellent coffee example (also worth reading in full) to show why the relative risk of having a heart attack within an hour of consuming a cup of coffee (1.5, or 50% increased risk) translates in real life to an absolute risk of one heart attack per 2 million cups of coffee.
Now that we’re all primed with statistical knowledge, I think we can risk reading through the table while sipping cups of coffee and listening to our tinnitus diminish and our hearts beat reassuringly. Happy International Coffee Celebration for Audiologists and their patients!


feature photo courtesy of University of Michigan