


Harvey Abrams PhD
“Peeling the Onion” is a monthly column by Harvey Abrams, PhD
“There is nothing wrong with change as long as it is in the right direction” – Winston Churchill
To date, the theme of my posts has focused on the two primary approaches to audiologic care – medical and rehabilitative. The rehabilitative approach recognizes adult-onset hearing loss as a chronic health condition similar, for example, to diabetes or heart disease, in that they share some common characteristics: they’re invisible, progressive, painless, and incurable, though manageable.
A Long Journey With Many Stages of Changes
Another important feature that hearing loss shares with other chronic health conditions is the journey individuals travel before they take action. A model of this decision-making process is described by the Health Belief Model (HBM) discussed in last month’s post.
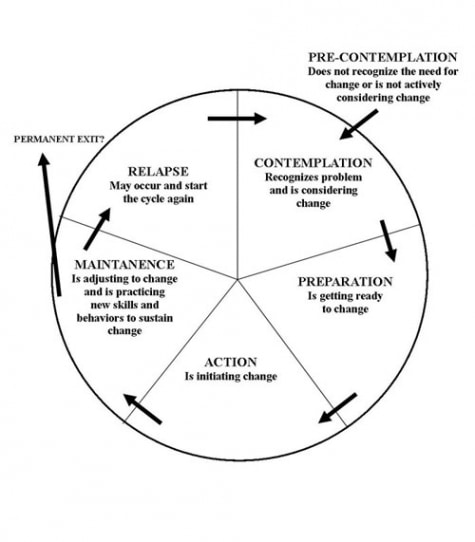
Fig 1. The Transtheoretical (Stages of Change) Model. from bsober.org
HBM can be considered a sub-set of a larger biopsychosocial model called the Transtheoretical Model (TTM) (Figure 1), also referred to as the Stages of Change Model. TTM was first proposed by Prochaska and DiClemente1 to describe a therapeutic approach to smoking cessation. The model has subsequently been applied to eating disorders and other conditions2345. The TTM model recognizes that behavior change is difficult and that most individuals progress (and sometimes, regress) through a 6-stage cyclical process.
These 6 stages of change are described as follows:
- Precontemplation (not ready): In this stage, individuals have no intention of changing anytime in the near future (e.g., 6 months) and tend to overestimate the negatives (costs) and underestimate the positives (benefits) associated with changing their behavior.
- Contemplation (getting ready): In this stage, individuals become increasingly aware of the positive attributes of changing their behavior and may intend to do so in the next 6 months; however, some may see the pros and cons of taking action as equal and their ambivalence may delay action for a considerable length of time.
- Preparation (ready): Here the individual is ready to take action in the near future (within the next month). They may have consulted with their physician, made inquiries among friends or conducted online searches.
- Action: In this stage, a specific behavior change has taken place (e.g., joining a gym, cutting down on cigarettes, joining an addiction support group).
- Maintenance: Actions at this stage are directed toward sustaining the change in behavior and reducing the risk of relapse. If relapse should occur, the individual may need to re-enter the cycle, and they may do this at any one of the previous stages.
- Termination: This stage describes the point at which the positive behavior change has become habituated and the risk of relapse is minimal.
Apply TTM to Audiology
What, then (need I ask?), does the TTM have to do with a rehabilitative approach to audiologic care? As we all know, on average, many years pass between the time an individual suspects they have a hearing problem and the purchase of their first hearing aids. What happens over those 5 years could easily be explained by the TTM.
Untreated hearing loss certainly does not rise to the level of risk of untreated addiction. Nonetheless maladaptive behaviors do occur as a consequence of untreated hearing loss, such as ineffective attempts at communication repair (e.g. “huh?”), avoidance of situations that previously were sources of enjoyment, social isolation, placing the burden on friends and family for successful communication exchange, etc.
Here then, are some examples of how the stages of TTM can be applied to an individual with hearing loss:
- Precontemplation: Mr. Smith is beginning to experience hearing difficulties (asking for repetition, having to turn up the TV), but has no intention of seeking help. All he knows about hearing aids is that they are expensive, his friends who wear them complain about how they make the background noise louder, and he has memories of his hearing-impaired uncle wearing a bulky, unattractive body aid that whistled all the time.
- Contemplation: Mrs. Smith is complaining about the volume of the TV being much too loud and his friends are remarking about how often he misunderstands what they say and how often they have to repeat themselves. Mr. Smith begins to check out information about hearing aids on the Internet and is impressed with their small size and technological sophistication (to include reducing whistling and background noise). He’s had his hearing screened by his primary care physician, which confirms what he has suspected for the past 5 years – he has a hearing loss.
- Action: Mr. Smith gets a recommendation from a friend who has had good results with her hearing aids and makes an appointment with a hearing care provider in his community. Following a positive experience, Mr. Smith decides to purchase a pair of hearing aids.
- Maintenance: As a result of his audiologist’s rehabilitative approach to hearing healthcare, Mr. Smith is provided with appropriate counseling, follow-up care, and post-fitting rehabilitation strategies that minimize his risk of relapse (i.e., not wearing his hearing aids and resorting to his previous maladaptive repair strategies).
- Termination: Following a year of successful hearing aid use, Mr. Smith is re-engaged into the world of sound and all of its associated benefits.
A more detailed description of the applications of the TTM or Stages of Change Model to hearing healthcare can be found at the Ida Institute.
This is Part 5 of the Peeling the Onion series. Click here for Part 1, Part 2, Part 3, Part 4, or Part 6.
References:
- Prochaska, JO & DiClemente CC (1983). Stages and processes of self-change of smoking: Toward an integrative model of change. Journal of Consulting and Clinical Psychology, 51, 390-395.
- Logue E et al. (2005). Transtheoretical model-chronic disease care for obesity in primary care: A randomized trial. Obesity Research, 13(5), 917-927.
- Callaghan RC et al. (2007). Does progressive stage transition mean getting better? A test of the Transtheoretical Model in alcoholism recovery. Addiction, 102(10), 1588-1596.
- Prochaska JO et al. (1994). The Transtheoretical Model of Change and HIV Prevention: A Review. Health Education Behavior, 21(4), 471-486.
- Johnson S et al. (2006). Transtheoretical model intervention for adherence to lipid-lowering drug. Disease Management, 9(2): 102-114.
Harvey Abrams, PhD, is Principal Research Audiologist at Starkey Technologies. Dr. Abrams has served in various clinical, research, and administrative capacities with Starkey, the Department of Veterans Affairs and the Department of Defense. Dr. Abrams received his master’s and doctoral degrees from the University of Florida. His research has focused on treatment efficacy and improved quality of life associated with audiologic intervention. He has authored and co-authored several recent papers and book chapters and frequently lectures on post-fitting audiologic rehabilitation, outcome measures, health-related quality of life, and evidence-based audiologic practice. Dr. Abrams can be reached at harvey_abrams@starkey.com


