

Brian Taylor, AuD
“Signal & Noise” is a bimonthly column by Brian Taylor, AuD.
Identifying and addressing the unmet needs of people with hearing loss means more than reducing costs (the Public Health Perspective) or improving devices (the Biomedical Perspective). The extent and limits of those approaches were covered in part 1. Today’s post suggests that we can meet people’s hearing needs better if we hand them the reins.
The Psychosocial Perspective
Aside from cost effects on hearing acceptance statistics, reports indicate low uptake may be the result of psychosocial factors, which are often overlooked. Recent studies suggest several factors, other than cost, associated with seeking help for hearing loss.
A 2014 retrospective study involving 307 adults aged 60 and older found that among the factors influencing help seeking for hearing loss were a declining ability to cope with hearing loss, greater levels of self-reported difficulties and social pressure to take action. Other research suggests that passive acceptance of hearing loss, stigma and the negative outlook of others with respect to hearing aid use may delay help seeking for those with a possible hearing loss.
Experts in the field point out seeking the assistance of a hearing care professional about a potential hearing loss should not be equated with a willingness to purchase hearing aids. In fact, a 2012 peer reviewed study suggested that when given a choice of interventions, some of which do not center on the provision of a device, about 40% of patients opt for the non-device option. Further, given that approximately 80% adults with hearing loss do not seek help during the first 50 to 10 years after noticing hearing loss suggests that beyond the introduction of lower cost technology, in-depth patient counseling and education are important considerations in solving the problem of the long delay in help seeking and use of hearing aids.
Time to Leave the Biomedical Model and Let Patients Set the Agenda
Regardless of your stance on the PCAST report and the underlying factors contributing to delays in seeking help and the poor uptake of hearing aids, clinicians would be wise to use more patient-centric communication. It would help the entire profession move beyond the limited, and perhaps stagnant, biomedical perspective that too often thinks all hearing difficulties can be solved with a better hearing aid or a more remarkable service experience with the professional.
At the same time, genuine patient-centric communication, which is a hallmark of the psychosocial perspective, would address the serious shortcomings of public health officials who believe the problem can be solved with a cheaper device sold directly to consumers. Today, early intervention and patient-centered communication, in which the patient is allowed to set the agenda is, as Shakespeare said, “more honored in the breach than the observance.” For example, Grenness and colleagues reported in a 2015 issue of JAAA that an astounding 83% of all information given by the audiologist throughout the patient consultation is biomedical in nature: we love to discuss the audiogram and hearing instrumentation.
As more Baby-boomers, who typically have a strong desire for direct involvement in their healthcare, enter the market for our services it is important we peel Harvey Abram’s onion and recognize their “stage of change” and “triggers to action”. Additionally, clinicians need to recognize that the vast majority of hearing loss in adults starts within the normal range and deteriorates slowly. We need to use technology to engage people early through self-screening and adaption of technology that helps in specific listening situations, which are often problematic for aging individuals with “normal hearing for their age.”
For those that adhere to a purely biomedical perspective, alternative interventions designed to help patients with essentially normal hearing or mild loss can be viewed as gateway products that may speed the journey to traditional hearing aid acceptance as a patient ages and needs more help.
Five Reasons Patients Seek Hearing Help
Recently, leading researchers, such as Gaby Saunders, Arlene Carson, Louise Hickson and Arianne Laplante-Levesque have begun to popularize the use of various models to describe the behaviors and attitudes associated with the chronic condition of age-related hearing loss. We can begin to infuse their work into our counseling approach with patients by addressing five key reasons why individuals, often waiting several years, finally decide to seek help from a hearing care professional. (By the way, none of these reasons have anything to do with cost). According to the experts the five reasons are:
- Have a support network (family, friends, trusted family doctor) who encourage them to seek assistance
- Have more severe symptoms (greater hearing loss)
- Current ability to cope with their condition is ineffective
- Does not expect to be stigmatized (judged, mocked or belittled) for seeking help
- Feels the condition has a significant impact of daily living
In a nutshell, these five areas of concern are known as the Health Belief Model. It is an essential part of our job to address each of these points during the face-to-face consultation with a patient, or in our interactions with the community. In the clinic, we can accomplish this by shifting from one-way dialogue about test results and technology to give-and-take conversations that unpack the emotional baggage associated with living for so long with a debilitating condition. Perhaps if we focused on counseling & intervention strategies that addressed these five areas, uptake for our products and services would be higher:
- Encourage early self-screening of hearing loss. Educate the community that even adults with normal audiograms may have difficulties with day-to-day communication, and intervention – beyond traditional hearing aids – can be helpful.
- Embrace the public health perspective through the judicious use of PSAPs and other hearables for patients with milder self-reported hearing difficulties. It also includes the use of community-based health workers to educate the entire population about the importance of hearing screening, the deleterious effects of hearing loss of adult onset and effective early intervention options.
- Provide emotional support. Discuss the importance and willingness of getting help while respecting the patient’s values and “stage of change”
- Offer unbiased educational information. Show the patient all of their possible solutions, including the advantages and limitations of each. This can be done with a visual aid like the one shown in Figure 1.
- Conduct a hands-on demonstration of various technology offerings. Allow patients to touch, feel and use various devices prior to purchasing them. In short, modernize your ALD display with hearables.
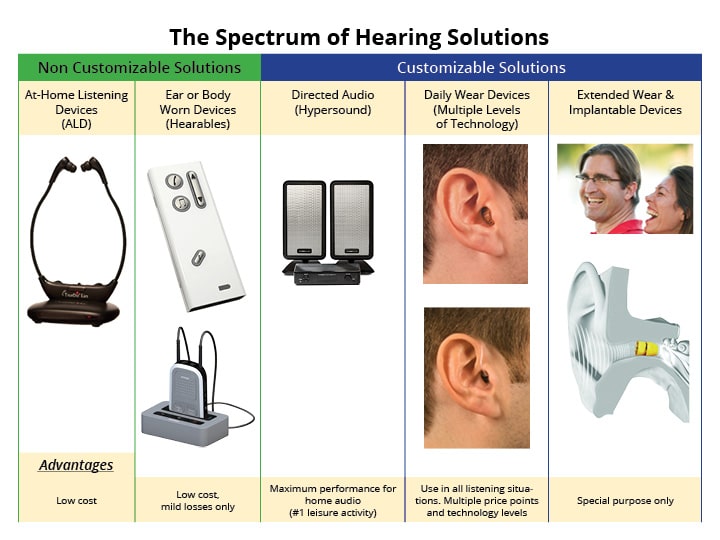
Figure 1. An example of a product education visual aid.
Finally, when authentic patient-centric communication and shared decision making are put into practice, as shown in Figure 2, individuals are more likely to feel that we addressed their needs and helped them – sometimes without even dispensing a product. At the end of the day it’s these humanistic communication skills, rather than our technical ability that will transcend our recent spats over the re-regulation of hearing aids.
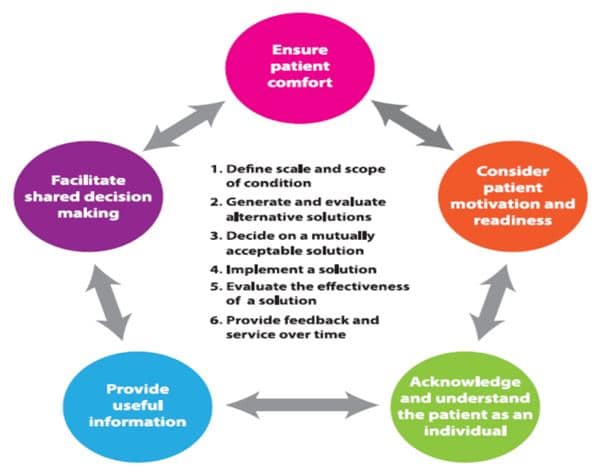
Figure 2. Patient-centric communication and shared decision making.
Juggling 3 Different Perspectives
That executive panel in part 1 of this post, representing the biomedical perspective, is the clinician’s ally, but hearing care professionals owe it to their patients to broaden their perspective on how to better meet the needs of those with hearing loss and communication difficulties stemming from it.
Keep your mind open to what all individuals with communication difficulties value. It may be something no one has yet to offer. The future of our profession hinges on our ability to juggle three different perspectives. The status quo – conducting a routine audiogram and fitting hearing aids on those that after several years of passive acceptance eventually find their way to our clinics – must change. It’s time to usher in a new era of clinical audiology that embodies all three perspectives.
Figure 2. A roadmap for patient-centric communication based on the work of Laya Poost-Faroosh, Louise Hickson, Caitlin Grenness and others
Brian Taylor, AuD, is Senior Director, Clinical Affairs, for Turtle Beach/Hypersound. He continues to serve as Editor of Audiology Practices, the quarterly publication of the Academy of Doctors of Audiology. During the first fifteen years of his career, he practiced clinical audiology in both medical and retail settings. Since 2005, Dr. Taylor has held a variety of leadership & management positions within the hearing aid industry in both the United States and Europe. He has published over 50 articles and book chapters on topics related to hearing aids, diagnostic audiology and business management. Brian has authored three text books: Fitting and Dispensing Hearing Aids (co-authored with Gus Mueller), Consultative Selling Skills for Audiologists, and Quality in Audiology: Design & Implementation of the Patient Experience. His latest book, Marketing in an Audiology Practice, was published in March, 2015. Brian lives in Golden Valley, MN with his wife and three sons. He can be reached at [email protected] or [email protected].
feature image courtesy of Cambridge in Color (edit)




