

Brian Taylor, AuD
by Brian Taylor
“Signal & Noise” is a bimonthly column by Brian Taylor, AuD
The May 30 installment of Signal and Noise “Good Audiology” series summarized the patient classification system devised by Stephens and Kramer a decade or so ago. It is a classification system that de-emphasizes the audiological assessment results and focuses on the emotions, attitudes and maladaptive behaviors of the individual and their communication partners.
A Fresh Approach for Unbundling
Their work laid the foundation for a fresher approach to patient care; an approach likely to gain traction in a future where the provision of unbundled counseling services will become popular.
To review, Stephens and Kramer devised a system based on four types of adult patients with hearing loss, with 80% to 90% of patients fitting into either the Type 1 or Type 2 categories. Here are their four patient categories:
- Type 1: Positively motivated without complicating factors
- Type 2: Positively motivated with complicating factors
- Type 3: Wants help, but rejects a key component of your recommendation
- Type 4: Denies any problems with hearing or communication
Determining Case Complexity
One of the challenges associated with adapting such a system is that the traditional audiological test battery, which works well for identification of ear disease when it is properly executed, has significant limitations for use in the Stephens & Kramer system. Besides the occasional asymmetrical hearing loss or poor word recognition scores, I can’t think of too many test results stemming from the traditional battery of tests that will help, say, differentiate between a Type 1 and Type 2 hearing loss.
There are, on the other hand, an abundance of non-audiological1 dimensions that contribute to differentiating a routine (Type 1) patient from the other three Types. Dimensions such as self-confidence, motivation and cognitive ability – areas beyond the degree of hearing loss – that oblige clinicians to expend more time and expertise addressing.
Surprisingly, much of the chatter and debate surrounding the creation of a direct-to-consumer device category has focused exclusively on degree of hearing loss as the sole indicator of complexity. That is, as I understand the argument, the worse an individual’s pure tone thresholds, the more crucial it is for that person to see a hearing care professional prior to using amplification.2 Although degree of hearing loss may have some value in necessitating the need to consult a licensed professional prior to purchase, it is the imprecise, somewhat fuzzy non-audiological dimensions that usually determine the complexity of a case.
A Call to Action
There are at least six dimensions of patient care that cannot be addressed from the traditional audiological assessment. Let’s refer to them as non-audiological or downstream components of care. Our ability to assess each of these components – either formally with a self-report or more objective screening procedure or through informal observation — is an essential part of patient care, requiring face-to-face interaction with a licensed professional. Each of these six dimensions has sufficient evidence suggesting it influences treatment outcomes3.
Here are the six downstream dimensions, along with a brief explanation:
- Cognition: The executive function (memory, language comprehension, etc.) of the individual.
- Physical Ability: The fine motor skills of the individual, particularly haptic ability.
- Attitude/Motivation: The general outlook of the individual toward life and completing new tasks or changing/modifying behaviors. When judged on a continuum the individual could be stubborn to compliant or extremely optimistic to extremely pessimistic.
- Family Support: Consistent contact with either a family member or close friend (communication partner. On the opposite side of the family support continuum would be social isolation.
- Self-confidence: A trust in one’s abilities and judgements to complete a task or modify a behavior
- Self-perception of hearing loss: An individual’s own opinion or awareness of their ability to hear and its associated handicapping condition. Oftentimes a clinician can assess self-perception of hearing loss by asking a scaling question (“On a scale of 1 to 10 with a ten being perfect hearing, how would you rate your overall ability to hear?”).
Clinicians could go to PubMed and identify several validated tests and questionnaires that measure each of these dimensions, but it is doubtful that many of these well-designed tools would be consistently used in the clinic.
However, just because a clinician doesn’t have time to administer, score and discuss several different metrics, doesn’t mean these important dimensions of patient care can be ignored. Given the looming direct to consumer sales of hearing aids, clinicians cannot let the perfect be the enemy of the good.
A Practical Way to Separate Routine from Complex
Even though audiologists informally observe all of these dimensions, to date, there is not a consensus on how to assess each of downstream dimensions of patient care. Here is a practical approach to sizing up these critical non-audiological dimensions of patient care with the goal being categorizing each patient into one of four patient Types using the Stephens & Kramer system.
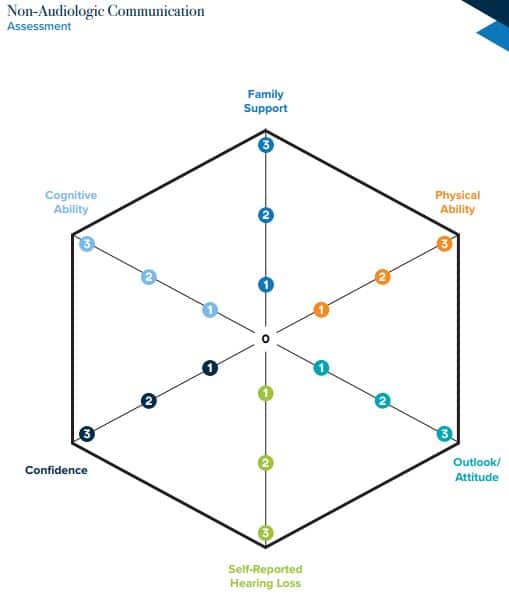
Figure 1. Communication Haxagram from Stephens and Kramer (2009)
While rank and file professionals wait for researchers to create the next generation of clinical tools, we cannot afford to idly stand by. One way to take action would be to use something like the Communication Hexagram shown in Figure 1.
The basic idea is that each of the six downstream dimensions could be assessed on a 0 to 3 continuum. The lower the number, the more problematic that particular dimension is judged to be by the clinician. Hence, a low overall score determines that an individual is deemed to be a complex case, requiring more time and/or expertise. Thus the complex case is charged more for services. Using the Communication Hexagram a perfect score would be 18. If the overall score is 12 or less, the patient could be classified as complex. Or, a score of 0 or 1 on any single dimension they classify a patient as complex. Trial and error would help us tweak these numbers, but intuitively it seems like a good starting point.
Jumping Off Points for Assessment, Triage and Assessment
Besides interpretation of the basic site of lesion audiological test battery, audiologists need to own the metrics and procedures associated with separating routine from complex cases. Work is already underway to create accurate cost effective systems that triage benign, age-related hearing loss from ear disease.4 Further work needs to be done to separate routine communication deficits that don’t require the intervention of a highly skilled audiologist from more complex cases that benefit from our expertise.
- The working definition of non-audiological dimensions are patient traits that are not determined by the routine audiological assessment of pure tone air and bone conduction audiometry, word recognition scores to ascertain best score (PB Max), acoustic reflexes, tympanometry and oto-acoustic emissions. See Jay Hall’s 2-part test battery series from June posted at Audiology Online.
- In a 2009 Otolaryngology-Head & Neck Surgery commentary, Halpin & Rauch of Mass Eye & Ear provide a compelling case for providing a generic, one-size-fits-all, flat frequency response for cases of severe cochlear damage. Their data suggests that a patient’s word recognition ability (conducted at two different intensity levels) determines the degree of damage and not the thresholds on the audiogram. This important bit of evidence has managed to fly under the radar as the OTC debate has raged on the past few years.
- Readers are encouraged to go to PubMed and enter hearing loss + each of the six dimensions listed above to get a flavor for the number of questionnaires, screeners and other tools used to assess each of these critical dimensions and how each contributes to treatment (hearing aid) outcomes.
- Samantha Kleindeinst and colleagues recently published an update on CEDRA – a consumer- driven questionnaire designed to cost effectively separate cases of ear disease from benign age-related hearing problems in adults. According to their recent paper, the current version of CEDRA would miss 15% of cases with ear disease and over-refer 53% of cases without ear disease. As they continue to refine this tool, keep in mind their work is a great example of how machine learning principles, likelihood ratios and risk scores are going to change the way we practice audiology in the near future.
References
Halpin C & Rauch SD. Clinical implications of a damaged cochlea: pure tone thresholds vs information-carrying capacity. Otolaryngol Head Neck Surg. 2009 Apr;140(4):473-6. doi: 10.1016/j.otohns.2008.12.021.
Stephens D & Kramer S. (2009). Living with Hearing Difficulties: the Process of Enablement. Hoboken NJ: Wiley.
Brian Taylor, AuD, is Senior Director, Clinical Affairs, for Turtle Beach/Hypersound. He continues to serve as Editor of Audiology Practices, the quarterly publication of the Academy of Doctors of Audiology. During the first fifteen years of his career, he practiced clinical audiology in both medical and retail settings. Since 2005, Dr. Taylor has held a variety of leadership & management positions within the hearing aid industry in both the United States and Europe. He has published over 50 articles and book chapters on topics related to hearing aids, diagnostic audiology and business management. Brian has authored three text books: Fitting and Dispensing Hearing Aids(co-authored with Gus Mueller), Consultative Selling Skills for Audiologists, and Quality in Audiology: Design & Implementation of the Patient Experience. His latest book, Marketing in an Audiology Practice, was published in March, 2015. Brian lives in Golden Valley, MN with his wife and three sons. He can be reached at [email protected] or [email protected].
feature image courtesy of Cambridge in Color (edit)


Excellent article, Brian. Those six dimensions of patient care are crucial in most effectively treating a person with hearing loss.