


Amyn Amlani, PhD
by Amyn Amlani, PhD
The uptake of traditional hearing aids—not just in the United States (US), but globally—has yet to reach its maximum potential. In a recent blog,1 it was reported that hearing aid uptake is highest in Norway (42.5%), the United Kingdom (UK; 41.1%), and Switzerland (38.8%), in which these devices are either fully (i.e., Norway, Switzerland) or primarily (i.e., UK) subsidized by each countries respective government. The US market, which is premised on capitalism, boasts an adoption rate of 30.2%.
Subsidized versus Open Markets
In the same blog, we reported on the estimated uptake growth in the US market for fully subsidize hearing aids versus improvements in the way we conduct our day-to-day business. Briefly, economic modeling in a fully subsidized climate revealed that the number of estimated users would increase by about 1 million new users. From a practical standpoint, this estimated growth appears constrained if we simply look at the 28% uptake in the Veteran’s Administration.2
This data suggests that many listeners fail to see the value in using amplification despite the fact that the product is provided at no cost.
Conversely, if the market remained capitalistic but improved its service delivery model, standard of care, rehabilitation/counseling efforts, etc., a 5% increase in demand function is expected to yield an estimated growth of about 2.5 million new users.1 In this blog, we take a candid assessment of the degree to which the value between provider-patient intervention/counseling influences hearing aid uptake.
Consumer Decision Model (CDM)
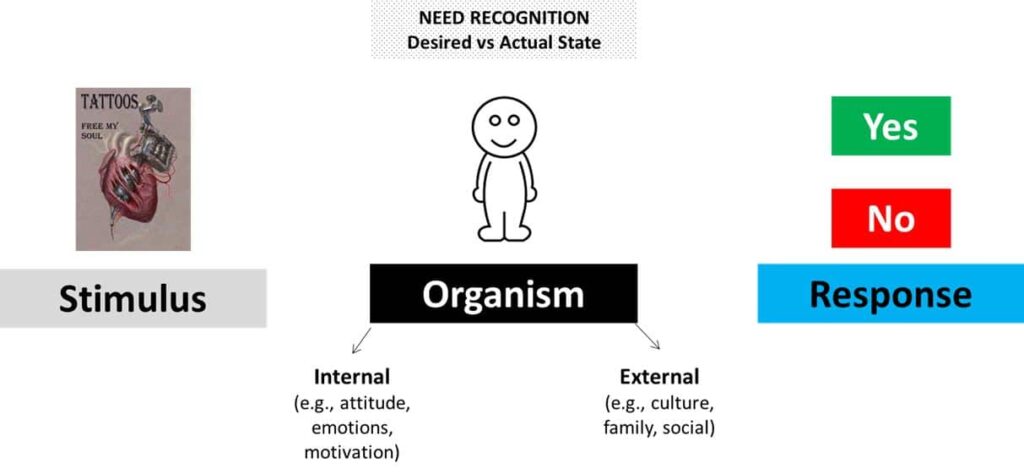
Figure 1. An example of the Stimulus-Organism-Response (SOR) in the CDM. See text for details.
To assess the value of provider-patient intervention/counseling, we utilized the Consumer-Decision-Making Model (CDM).3 The CDM is a neo-behavioral psychological approach that accounts for an individual’s psychological and cognitive approach toward a product or service. Specifically, this model is premised on the stimulus-organism-response (SOR) approach, which is illustrated in Figure 1.
In the example, the stimulus presented to the organism (i.e., individual) is an ad for a tattoo. The ad motivates psychological and cognitive information processing, which is influenced by intrinsic (e.g., attitude, emotions, motivation) and extrinsic (e.g., culture, family, social) factors. Need recognition is where the decision-making process is moderated by the individual’s desired (i.e., expected) state and their actual (i.e., current) state. A positive (i.e., purchase) response only occurs when the desired state from the stimulus is anticipated to improve the individual’s actual state.
Study Characteristics
Using the model above, we posed the following question to a cohort of 1273 older adult listeners with self-perceived hearing loss before and after their initial appointment to have their hearing sensitivity evaluated between October 2015 and December 2016:
In your opinion, the profession of audiology is best classified under the heading of (a) medical, (b) rehabilitation, or (c) consumer electronics?
Each listener agreed to undergo an evaluation of their hearing sensitivity and made their own appointment with a local provider of their choice. Fourteen days before their appointment, participants were asked to provide a response to survey questions about their desired expectations regarding the facility, front desk staff, and the provider. Data revealed that the average listener provided responses 7.6 days before their appointment (SD = 3.8).
Within 14 days after their appointment (mean = 3.3 days, SD = 2.1), participants provided their responses to the same survey questions about their actual perceptions of the facility, front desk staff, and the provider.
With respect to the question noted above, Table 1 shows the following percentage of respondents reported that audiology was best classified as:
|
Professional Classification of Audiology |
Pre-Appointment |
Post-Appointment |
|
A. Medical |
23% |
9% |
|
B. Rehabilitation |
63% |
28% |
|
C. Consumer Electronics |
14% |
63% |
In addition, we asked respondents whether they were interested in hearing aid technology to overcome their listening difficulties before and after their initial appointment. The data, shown in table 2, revealed:
|
Interest in Hearing Aid Technology |
Pre-Appointment |
Post-Appointment |
|
Yes |
67% |
22% |
|
No |
33% |
78% |
Conclusion
The outcomes from this study suggest that:
- listeners with self-perceived hearing difficulties have a positive expectation towards having their hearing difficulties remediated prior to their appointment.
- At some point during the appointment, this positive expectation is reassessed, and in many cases, reduced to the point where the actual state is equal to or better than their expected state.
- This results in a negative response towards the professional and the technology, which appears to be influenced by the provider.
Because we are still analyzing the dataset, it remains unclear as to how the provider is negatively influencing the uptake process. We hope to provide this information in a future installment.
Figure 1. An example of the Stimulus-Organism-Response (SOR) in the CDM. See text for details.
References
- Amlani AM. (2016, August 31). Consumers, Consumers…Where art thou? HearingHealthMatters.0rg
- Yeuh B, Collins MP, Souza PE, Boyko EJ, Loovis CF, Heagerty PJ, Lie CF, Hedrick SC. (2010). Long-term effectiveness of screening for hearing loss: The screening for auditory impairment-which hearing assessment test (SAI-WHAT) randomized trial. J Am Geriatr Soc, 58:437-434.
- Amlani AM. (2016). Application of the Consumer Decision-Making Model to hearing aid adoption in first-time users. Sem Hear, 37: 103-119.
Amyn M. Amlani, Ph.D., is Professor and Chair of the consortium program in Audiology & Speech Pathology between the University of Arkansas for Medical Sciences and the University of Arkansas at Little Rock. Dr. Amlani holds the B.A. degree in Communication Disorders from the University of the Pacific, the M.S. degree in Audiology from Purdue University, and the Ph.D. degree in Audiology/Psychoacoustics (minor in Marketing and Supply Chain Management) from Michigan State University. His research interests include the influence of hearing aid technology on speech and music; economic and marketing trends within the hearing aid industry; and playing bass guitar in various heavy metal cover bands. Email: AMAmlani@uams.edu
*title image courtesy wikimedia commons



{kind=link}
Since the patients were able to see a local provider of there choice, I cannot help but wonder if they were asked to specify the role of that provider. Were they seeing audiologists, hearing aid dealers, a mix?
Tim:
Great question. The findings described for patients seen by an only audiologist. I have data for hearing instrument specialists, which was not reported in this blog.
-Amyn
Amyn, this is a great study that provides objective evidence that the provider is the key to patient acceptance of their problem and treatment. Studies indicating that the return rate is lower and the number of office visits are less if you do real ear and/or aural rehab are based on invalid and unreliable reports. The main reason patients agree to treatment, and decide to purchase and keep hearing aids, is the provider. Just video tape the patient-provider sessions and any good hearing care provider can tell you after watching why the patient did not agree to treatment and/or returned the hearing aids. Keep up the great work!
The summary and data posted appears to say the opposite though?