
By Barry Freeman, PhD, and Ian Windmill, PhD
The past few decades have been dominated by efforts to control healthcare costs while improving affordability and access to quality care. Hearing care is no exception as demonstrated by the reports of the 2016 NASEM Committee on Accessible and Affordable Hearing Health Care for Adults and the 2016 Report from the President’s Council of Advisors on Science and Technology (PCAST, 2015). Both groups recommended steps necessary to improve accessibility and affordability of hearing healthcare for adults. Similarly, The Department of Health and Human Services (HHS) HealthyPeople 2020 has among their goals an increase the number of adults who have had a hearing examination, tinnitus evaluation, and the number of adults with balance or dizziness who have seen a professional.
Yet, despite these efforts, Medicare policies place financial and onerous burdens on beneficiaries which can compromise access to quality hearing and balance care.
Attention to hearing and balance problems have been heightened with a goal of reducing incidence while improving management and treatment. Pre-Medicare adults with commercial insurance and even many adults with Medicare Advantage plans have health insurance that provide their beneficiaries with direct access to hearing and balance care.
Most, if not all, of these insurance plans have removed the obstacles of requiring a physician referral to access Audiology services that are inherent in the traditional Medicare system which is more complex, expensive, and less accessible to their beneficiaries.
The government sponsored report, Hearing Health Care for Adults (2017) recommended examining “the Medicare requirement for physician referral for diagnostic hearing testing.” The obstacles posed to Medicare beneficiaries accessing the hearing care system include, “a lack of access to medical providers due to financial barriers, appointment wait times, or transportation difficulties.” The report panel also noted that “studies have demonstrated that the overall ear disease prevalence in the population of adults with age-related hearing loss is low and that patient populations in health systems that do not require a referral do not have higher rates of missed disease (Zapala et al., 2010; Zapala et al, 2015, Blazer et al, 2016). These conclusions validate earlier studies demonstrating the cost-effectiveness of providing patients with hearing disorders direct access to audiologists would reduce costs without compromising the quality of patient care (Hall, Freeman, and Bratt, 1994; Bratt, Freeman, Hall and Windmill, 1996; Yaremchuk, Schmidt, and Dickson, 1990).
The purpose of this paper is to evaluate the costs incurred in the year 2017 by Medicare and their beneficiaries who were referred for hearing care services.
Access to Audiology Services by Medicare Beneficiaries
Bratt et al. (1996) described three models of entry and delivery of hearing care services based on their effectiveness, efficiency, and viability. In the first model, patients present to a physician, most often the primary care physician (PCP) with a complaint of hearing problems. If the referral is made to a PCP, the patient then may be referred to an otolaryngologist who refers to the audiologist. This is a three-step process where at least 80-90% of patients did not have a medically/surgically treatable condition.
In the second model, the physician may refer directly to an audiologist, thus bypassing the intermediary visit to a second physician.
Subsequently, the 10-20% of patients with a medical/surgically treatable disorder are identified by the audiologist and are referred for medical management. Most private and other government insurance programs (e.g., Department of Veteran Affairs, Federal Employee Health Benefit Plans), have adopted a third model where patients have direct access to audiologists.
For 80-90% of patients with direct access, that would be the only step required in the evaluation and management of these patients. The remaining 10-20% would require a medical/surgical referral. The audiologist has the knowledge and skills necessary to identify these patients and make the appropriate referral.
Freeman and Lichtman (2005) applied the models of entry to hearing care and completed a cost-savings analysis based on Part B National Summary Data File (Previously known as BESS) from the year 2000 for Audiology Services. They concluded that permitting Medicare beneficiaries with a complaint of hearing loss direct access to audiologists would potentially result in significant cost-savings to Medicare.
Cost Analysis for Direct Access to Audiology Services
The purpose of this paper is to review the estimated costs associated with the Medicare physician-referral requirement to access Audiology services using published data from 2017 from the Centers for Medicare and Medicaid (CMS) Part B National Summary Data File previously known as BESS.
Current procedural terminology (CPT) codes are utilized by providers to describe their clinical procedure and by third-party payers to reimburse the provider. These codes allow healthcare providers to accurately bill for services provided to a patient. As a condition of reimbursement for audiology services, Medicare requires beneficiaries to have a physician referral prior to all reimbursed audiologic services.
Physicians have a choice of Evaluation and Management (E/M) CPT codes for their office visits and it is not possible to determine exactly which code was used by physicians prior to referring patients for Audiology services. Therefore, for this analysis, it was assumed that physicians selected from among the CPT codes 99201-99205 prior to referring Medicare beneficiaries for Audiology services. Figure 1 (below) summarizes the number of authorized physician visits and payments for evaluation and management codes paid by CMS to physicians in 2017 for all Medicare patients. Based on this data, Medicare authorized $3.6B to be paid to physicians for 27m Medicare patients, or an average CMS reimbursement of $139.02 for a physician office visit in 2017.
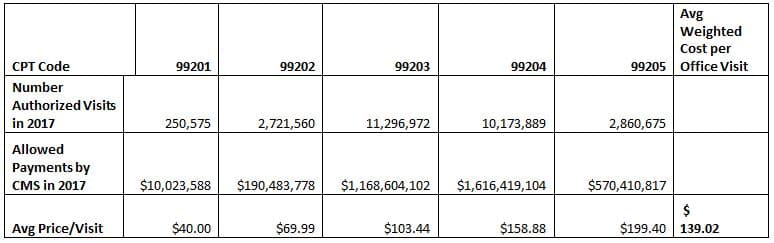
Figure 1. 2017 Medicare Authorized Visits for E/M CPT codes for physician office visits.
Audiology Services
Audiologists provide diagnostic and treatment services for hearing and balance disorders, and these results generally are interpreted with consideration to the pure tone audiogram. Therefore, it was assumed for this analysis that all patients referred by a physician for an audiology evaluation received a pure tone evaluation.
For the purposes of this paper, the CPT codes 92552 (air conduction threshold), 92553 (air and bone conduction threshold), and 92557 (comprehensive evaluation) were used to project the total number of patients referred to audiologists by physicians in 2017. The authors recognize that this is a conservative approach to project financial cost-savings and could potentially underestimate Medicare costs and potential cost-savings.
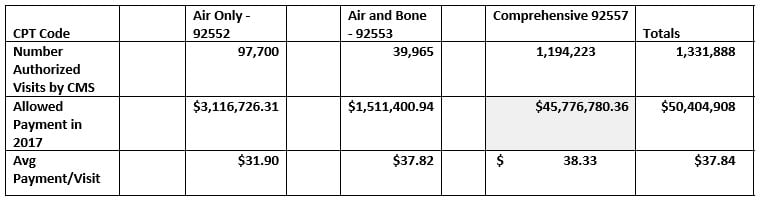
Figure 2. Summary CMS Payments for Audiology Services in 2017 for Beneficiaries on Traditional Medicare
As summarized in Figure 2, Medicare paid $50.4m for the more than 1.33m Medicare beneficiaries that were referred for a pure tone evaluation in 2017.
Figure 3 presents a hypothetical example of the costs associated with Model 1 presented by Bratt et al (1996) where all beneficiaries first visited their PCP, were then referred to an ENT physician, and then were referred for an audiology evaluation. It is clear this is an expensive model that may cost the government in excess of $457.7m or an average of $343.68 per patient for the 1.33m Medicare beneficiaries referred for a pure tone evaluation. In addition, since beneficiaries are required to pay a 20% co-pay, the patients have the burden of paying an aggregate of $91.6m or $68.74 out of pocket per referral for a hearing evaluation.

Figure 3. Estimated costs to Medicare if all beneficiaries followed the model of first visiting their Primary Care Physician who then referred to an Otolaryngologist (ENT) and then to Audiology with 20% patients having a condition that required medical follow-up..
In the second entry-model the patient is referred directly for audiology services by a physician, bypassing the second physician visit. As shown in Figure 4, the costs of Audiology services remain unchanged but total costs are reduced from an estimated $457.7m to $272.6m, or from an average cost per beneficiary of $343.68 to $204.66, due to the elimination of a second physician visit. Again, the Medicare beneficiary must pay a 20% co-pay of $40.93 per audiology referral or an aggregated $54.5m of the total expenses.

Figure 4. Estimated costs to Medicare if all beneficiaries followed the model of first visiting a physician who then referred directly to Audiology with 20% patients having a condition that required medical follow-up.
For more than a decade, there have been legislative and administrative efforts to convince CMS to amend their current physician referral requirement for Medicare beneficiaries to access audiology services. A majority of private and other government health insurance programs have found this approach to be cost-effective without compromising quality of care.
Staying with the models presented previously, Figure 5 summarizes the costs to Medicare if audiologists were permitted direct access to patients and referred 20% of these patients for physician management.

Figure 5. Estimated costs to Medicare if all beneficiaries first visited an audiologist and 20% were found to have a condition that required physician management.
Whereas the first model costs Medicare an average $343.68 per beneficiary and the second model would reduce these costs to $204.66, direct access would cost on average $65.64 per beneficiary as presented in Figure 6.
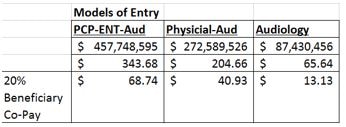
Figure 6. Comparison of costs associated with different models of entry to audiology services.
Comments and Conclusions
The Medicare data is clear. There are significant costs associated with the current system of entry to hearing health care. If beneficiaries choose to enter through the traditional Medicare model, then they are left with significant co-pays increasing their out-of-pocket costs, appointment wait times for physician visits prior to the referral for audiology services, plus costs associated with transportation, days-off from employment, or other personal commitments. The literature often mentions factors like stigma, cosmetics, and costs as barriers to entering the hearing care system. NASEM noted the disadvantages of the current Medicare system include “lack of access to medical providers due to financial barriers, appointment wait times, or transportation difficulties.”
Among factors used by the government and the insurance industry to measure the effectiveness of their plans and programs are an assessment of Opportunity Costs. These are costs or benefits individuals miss when they choose one alternative over another. Medicare beneficiaries, of which an estimated 30-50% have a communicatively handicapping hearing loss and co-morbidities associated with the hearing loss (Kleindienst et al, 2016; Zapala, 2015; Abrams, 2017) must make a choice between entering the existing Medicare system which is expensive and cumbersome, taking an alternative route where they may be evaluated for a medical device but not necessarily for the causes and treatment alternatives, or they may choose to not enter the system at all and live with their untreated handicap. They may need to make a choice between several mutually exclusive alternatives and hope that the costs incurred by their choice are not greater than the costs of missing the benefits of quality hearing care.
References:
- Abrams, H. Hearing loss and associated comorbidities (2017). Hearing Review, 24:12, 32-35.
- Blazer, D., Domnitz, S., Liverman (editors) (2016). Hearing Healthcare for Adults. National Academies of Sciences, Engineering, and Medicine. National Academies Press, Washington, DC.
- Freeman, B. and Lichtman, B. (2005). Audiology Direct Access: A cost savings analysis. Audiology Today, October 17:5, 13-14.
- Hall, J., Freeman, B., and Bratt, G. (1994). Audiology in healthcare reform: perspectives on
- models and medical referral guidelines. Audiology Today, 6, 16-18.
- Bratt, G., Freeman, B., Hall, J., Windmill, I. (1996). The audiologist as an entry point to
- healthcare: models and perspectives. Seminars in Hearing, 17:3, 227-234.
- Freeman, B. (1999). The reimbursement system: from managed care to Medicare. Seminars
- in Hearing, 20:2, 97-100.
- Kleindienst, S., Dhar, S., Nielsen, D, et al (2016). Identifying and Prioritizing Diseases Important for Detection in Adult Hearing Health Care. American Journal of Audiology, 25:224-231.
- PCAST (2015). Aging America and Hearing Loss.
- Yaremchuk, K., Schmidt, J., and Dickson, L. (1990). Entry of the hearing impaired into the
- healthcare system. Henry Ford Hospital Medical Journal, 38, 13-15.
- Zapala, DA, Stamper, G.C., Shelfer, J.S. et al. (2010). Safety of audiology direct access for Medicare patients complaining of impaired hearing. J. American Academy of Audiology 21 (6): 365-379.
- Zapala, DA, Lundy, L., Kleindienst, S, et al (2015) Development of a disease surveillance outcome measure for hearing healthcare. Paper presented at American Auditory Society Meeting, Scottsdale.
**A downloadable PDF version of this article can be obtained here: Hearing Care Direct Access Analysis
About the Authors:
 Ian Windmill, PhD, and Barry Freeman, PhD, are past presidents of the American Academy of Audiology.
Ian Windmill, PhD, and Barry Freeman, PhD, are past presidents of the American Academy of Audiology.



Hearing loss is a serious invisible disability. Purchasing a hearing aid more information and care is needed when choosing hearing aids. One size does not fit all. The Hearing Loss Association of American gave me the information I needed when I purchased my hearing aids (one for each ear). Hearing aids are not as easy to fit like eyeglasses. Hearing loss labels people as not too smart or seniors having dementia. I have been hard of hearing since 1940,