
by Brian Taylor
“Signal & Noise” is a bimonthly column by Brian Taylor, AuD
“The handshake of the host affects the taste of the roast”
–Benjamin Franklin

Brian Taylor, AuD
Query any hearing healthcare provider and she is likely to say she practices patient centered care1. The concept of patient centered care is a broad one, but one basic tenet of it is the patient sets the agenda for what’s covered during the appointment with guidance from the provider. For example, there is evidence suggesting patients have a greater acceptance of an intervention when they are offered an opportunity to choose from a range of options (La Plante-Levesque, et al 2012).2
Many providers believe they are practicing patient centered care, but research tells a different story. There are several studies indicating audiologists are perceived by patients as overly focused on technology and even emotionally distant. If these studies reflect reality, one could say most providers are practicing what is best termed “product centered care.”
In a series of published reports, Grenness and her colleagues at the University of Melbourne and University of Queensland analyzed dozens of appointments between adult patients and an audiologist. Their analysis suggests audiologists tend to control their interactions with patients. They found many patients raised concerns about the emotional and social consequences of their hearing loss only to be rebuffed by the audiologist who wanted to steer the conversation back to hearing aid technology and test results.
In one study they found that less than 5% of utterances of the audiologist addressed an emotionally-related topic initiated by the patient. Given the social and emotional consequences associated with hearing loss, such as frustration, annoyance and embarrassment, this is a missed opportunity to engage with patients on a deeper, more meaningful level.
The inability of many audiologists to emotionally connect with their patients is even more problematic when you consider the imminent deregulation of the dispensing process3. Soon it will be possible for a substantial number of individuals to purchase self-fitting hearing aids, and only find their way to an audiology clinic when they have a problem that cannot be adequately addressed through a smartphone app with an algorithm that uses artificial intelligence (AI) to solve it. As a profession we must plan for a day when a patient’s hearing aid problem can be solved with AI and machine learning, and we are left to address the social and emotional complexities of hearing loss that remain. If the work of Grenness and colleagues is a guidepost, most audiologists are ill-equipped to address the challenges associated with the psychosocial aspects of hearing loss.
The 2018 series of Signal & Noise posts hope to serve as a reminder that no matter how vital hearing aid technology is to patient outcomes, adults with hearing loss expect improved social and emotional well-being from their intervention from audiologists. More than simply learning how to use hearing aids, they want reduced annoyance, frustration and anxiety during communicative interactions; they desire to be more socially engaged and active; they want less stress associated with communication. For many individuals coping with hearing loss, these outcomes cannot be achieved unless they gain a trusting relationship with a licensed professional. Signal & Noise will tackle these issues and discuss how audiology needs to adapt if the profession wants to thrive in the era of self-fitting OTC devices, managed care and big-box retail.
A secondary goal of the upcoming Signal & Noise columns is to show examples of innovation in a more broadly defined way. Even though we have come to expect incremental progress with respect to hearing aid innovations, innovations can and do occur around the service experience. Innovations are not confined to microchips and software.
Audiology Best Practices and Best Principles are Needed
Let’s examine a concept that’s been around for more than 25 years, but worthy of a revisit4. It is the Progression of Economic Value. It is a good example of how hearing healthcare professionals need to look beyond clinical best practices and apply best principles that come from other professions. In the case of the Progression of Economic Value, it has been successfully applied in retail, education and other healthcare businesses.
Notice in Figure 1 (below) there are five distinct levels of value. Starting at the bottom left of the Figure, there are commodities, which are often literally extracted from the ground. Commodities are usually the raw materials used to make a product or good. In hearing care, commodities are the fungible components inside the hearing aids. Components from various manufacturers could be substituted for one another, and as long as they are working within a pre-determined specification, no one is likely to notice the difference.
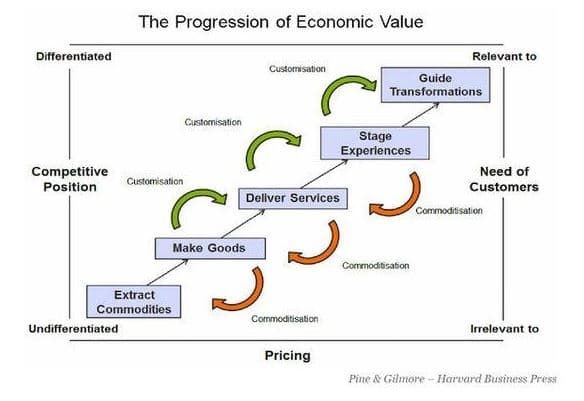
Figure 1. The Progression of Economic Value, Pine and Gilmore, 1993.4
The next level of value is goods. Take the hearing aid out of its packaging, place it on the ear, program and adjust it. Although software allows for customization of the hearing aid to the individual’s hearing loss, you can buy a high-quality device from many places: It can be purchased on-line, through the mail or in a clinic, often with minimal involvement from a provider.
Next, provide a service that helps people learn how to use their hearing aid and acclimate to their hearing aids, and you have reached the next level of value: An intangible service. A bit harder to measure and define, compared to a commodity or good, audiologists deliver services when they patiently teach patients how to insert and remove their instruments or counsel the patient of learning how to listen with hearing aids.
As we move up the ladder of value, customizing a service by designing or staging a series of memorable events moves us into the experience bucket. If services are delivered, experiences are staged4. For the audiology practice this means creating a series of memorable touch-points that engage the patient emotionally5. Provide those hearing aid counseling sessions in a memorable way using colorful brochures and effective communication skills, and you have likely created an experience.
*Click here for Part 2
References:
- In 2015 the Institute of Medicine defined patient-centered care as: “Providing care that is respectful of, and responsive to, individual patient preferences, needs and values, and ensuring that patient values guide all clinical decisions.”
- Laplante-Levesque, A, et al (2012) “What makes adults with hearing impairment take up hearing aids or communication programs and achieve successful outcomes?” Ear and Hearing. 33, 79-93..
- According to the January 2018 Bernstein Report, the FDA looming OTC regulations are likely to deregulate the hearing aid sales & distribution process. This means that rather than buy hearing aids from a licensed professional, a growing number of individuals will buy hearing aids direct from the manufacturer (or from an on-line distributor) and visit an audiologist for follow-up service. One possible by-product of a deregulated sales & distribution is the unbundling of service provisions from the sale of the product.
- The first edition of the Experience Economy by James Gilmore and Joe Pine was published in 1993. Their book introduced the concept of the Progression of Economic Value using birthday cakes and coffee.
- The book Quality in Audiology has a chapter describes how a practice to can stage memorable patient experiences and how these experiences might contribute to superior patient outcomes with hearing aids.
Brian Taylor, AuD, Brian Taylor is the director of clinical audiology for the Fuel Medical Group. He also serves as the editor of Audiology Practices, the quarterly journal of the Academy of Doctors of Audiology, and editor-in-chief of Hearing News Watch for HHTM. Brian has held a variety of positions within the industry, including stints with Amplifon (1999-2008) and Unitron (2008-2015). Dr. Taylor has more than 25 years of clinical, teaching and practice management experience. He has written and edited six textbooks, including the third edition of Audiology Practice Management (Thieme Press) which will be published in 2018. He lives in Minneapolis, MN and can be reached at [email protected]
*feature image courtesy of Cambridge in Color



Great article. Looking forward to Part 2.