
Hearing Healthcare Market Development Column
During the early months of the coronavirus pandemic, Sonova USA introduced to hearing care professionals (HCPs) a fully digital service delivery model for its Phonak brand. Patient use of the online hearing test, the gateway to care, skyrocketed during this period. However, very few HCPs implemented the fully digital model in their practices.
Phonak’s experience demonstrates the opportunities and challenges of implementing digital healthcare to an ecosystem of independent clinicians. (Disclosure: Auditory Insight has consulted with Sonova on hearing healthcare market segmentation and comorbidities with hearing loss.)
Phonak’s fully digital service delivery model
Phonak created its digital service delivery model for use by HCPs during times of extreme social distancing. “We wanted to avoid that [patients] had to delay that help for months and months,” explained Christine Jones, Vice President of Audiology at Sonova USA, in a video interview.
Phonak’s clinical guidelines recommend that HCPs establish hearing aid candidacy and then pre-fit the hearing aids using estimated hearing thresholds from the Phonak online hearing test (or a valid audiogram if available).
After shipping the hearing aids and setting up remote support with patients, HCPs perform in-situ hearing testing to confirm the audiometric estimates.
Jones stressed, however, that “we also recommend [for patients], when it is an acceptable risk, to come in and be seen for a face-to-face visit” for a full diagnostic evaluation, including otoscopy and testing for conductive hearing loss, which cannot be detected with a traditional tone test. Online hearing tests are distinct from a full diagnostic exam conducted by an HCP in accordance with state regulations.
The role of online hearing testing and Audiogram Direct
For new patients, the online hearing test plays a pivotal role in the fully digital service model. Jones reported that “a couple hundred providers have the e-screener embedded in their website,” with the number steadily growing. During the pandemic, Sonova upgraded the online test to assess more frequencies, providing a more complete picture of the patient’s hearing loss. In order to improve validity, the test pivoted to asking patients to characterize their headphones from four possible choices, as shown in the graphic below:
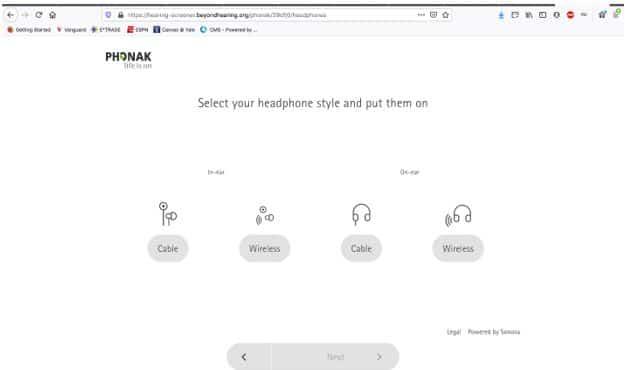
From March to mid-August 2020, patient use of the online hearing test grew by a meteoric 500%, according to a follow-up email from Jones, also noting that “currently several hundred people complete the [test] online each week.”
Along with the online hearing test, Audiogram Direct, Phonak’s in-situ hearing testing technology, enabled the direct service delivery model. In June 2020, Phonak released results of a retrospective study comparing the results of standard audiograms versus Audiogram Direct, which Jones explained “has been embedded in our software for over a decade.” The study concluded that the two methods produced differences of only 1.5 dB HL or less in outcomes for most frequencies, with the exception of 250Hz (-3.2 dB), 500 Hz (-2.4 dB), and 6000 Hz (4.2 dB).
Although most of the 100,000 plus data points came from fittings in Germany, in June 2020, Sonova USA replicated the findings with 24 subjects at their research center by putting the subjects through the entire digital service delivery model.
Audiogram Direct is “a very robust starting place for a hearing aid fitting,” Jones concluded.
Impact of the fully digital model on hearing aid sales
During the pandemic, did this new service model help Phonak turn prospects into users? “We didn’t see that happen a lot,” reported Thomas Lang, Vice President of Marketing, Sonova USA in a video interview. “It was too much of a job” for HCPs to transform their face-to-face delivery models into a fully digital model in the space of a few months.
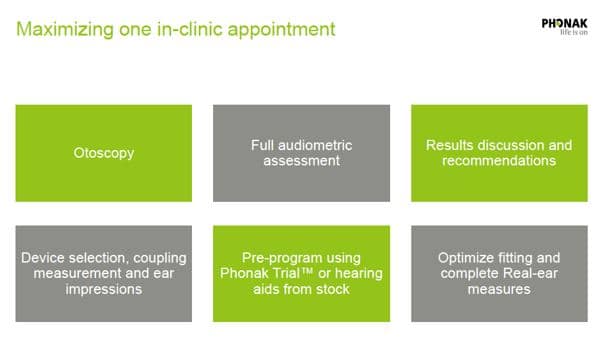
For the near-future, Phonak is recommending its blended service delivery model to HCPs. In the blended model the HCP combines services that used to be spread out over multiple visits into one longer appointment, from a diagnostic hearing exam through real-ear measures, as shown in the graphic below. “I don’t think a lot of people are going to follow that totally digital journey anymore because most places have loosened up a bit,” Jones said. “We know how to control risk, certainly in medical practices.”
Both Jones and Lang emphasize that patient needs should drive the ultimate configuration of the service model. For example, the Phonak guidelines identify a “modern, ‘tech-savvy’ client,”—about one-fifth of the Phonak base, Lang estimated—who would benefit from conducting their case history, goal setting, and post-fitting instruction via video calls.
However, Lang sees work ahead. “I often hear [clinicians] say, ‘No, my patients cannot handle e-solutions.’ Tailoring solutions based on patients’ needs “seems to be a concept which is not fully understood yet.”
However, with the baby boomer generation coming of age, Lang sees the patient segment valuing digital and at-home care growing. “There is no reason to believe why hearing healthcare should not be affected by the digital revolution” that is transforming overall healthcare, Lang concluded. “The fundamental drivers, which are convenience, empowerment, and maybe at some point cost pressure,” also apply to our industry.
**Disclosure: The author discloses that her company consults with hearing device manufacturers and pharmaceutical hearing healthcare companies.
 Nancy M. Williams is President of Auditory Insight, a boutique consultancy advising leaders on transforming hearing healthcare. Nancy partners with senior leaders of pharma and device companies to develop successful commercialization strategies based on deep insight into patient needs, practical understanding of clinical behaviors of audiologists and ENTs, and unique viewpoints on how hearing healthcare is evolving. She holds an MBA from Harvard Business School and a B.A. from Stanford University in Quantitative Economics, both with distinction.
Nancy M. Williams is President of Auditory Insight, a boutique consultancy advising leaders on transforming hearing healthcare. Nancy partners with senior leaders of pharma and device companies to develop successful commercialization strategies based on deep insight into patient needs, practical understanding of clinical behaviors of audiologists and ENTs, and unique viewpoints on how hearing healthcare is evolving. She holds an MBA from Harvard Business School and a B.A. from Stanford University in Quantitative Economics, both with distinction.



