
WASHINGTON, DC—If you or a loved one experiences sudden hearing loss (SHL) in one or both ears, getting a prompt and accurate diagnosis—and treatment, if necessary–is important in reducing the chance that the loss will become permanent.
So says the American Academy of Otolaryngology-Head and Neck Surgery Foundation (AAO-HSNF) in its new Clinical Practice Guideline on Sudden Hearing Loss (SHL) published March 1 as a supplement to Otolaryngology-Head and Neck Surgery.
SHL is a frightening condition that may result from a variety of causes and that most often prompts urgent medical care. The foundation’s guideline provides evidence-based recommendations for the diagnosis, management, and follow-up of adults who present with SHL.
According to the foundation, prompt, accurate recognition and management of sudden sensorineural hearing loss (SSNHL), a subset of SHL, may improve hearing recovery and patient quality of life. SSNHL affects 5 to 20 per 100,000 people, with about 4000 new cases a year in the United States.
The guideline is intended to help any clinician who may encounter patients with SHL. By focusing on opportunities for quality improvement, the guideline seeks to improve diagnostic accuracy, facilitate prompt intervention, decrease variations in management, reduce unnecessary tests and imaging procedures, and improve hearing and rehabilitative outcomes for affected patients.
Sudden Hearing Loss Clinical Recommendations
Among the main recommendations in the guideline are:
(1) Prompt and accurate diagnosis is important: (a) Sensorineural (nerve) hearing loss should be distinguished clinically from conductive (mechanical) hearing loss. (b) The diagnosis of idiopathic sudden sensorineural hearing loss (ISSNHL) is made when audiometry confirms a 30-dB hearing loss at three consecutive frequencies and no underlying condition can be identified by history or physical exam.
(2) Unnecessary tests and treatments should be avoided: (a) Routine head/brain CT scans, often ordered in the ER setting, are not helpful and expose the patient to ionizing radiation. (b) Routine, non-targeted, laboratory testing is not recommended.
(3) Initial therapy for ISSNHL may include corticosteroids.
(4) Follow-up and counseling is important: (a) Physicians should educate patients with ISSNHL about the natural history of the condition, the benefits and risks of medical interventions, and the limitations of existing evidence regarding efficacy. (b) Physicians should obtain follow-up audiometry within six months of diagnosis for patients with ISSNHL. (c) Physicians should counsel patients with incomplete hearing recovery about the possible benefits of amplification and hearing assistive technology and other supportive measures.
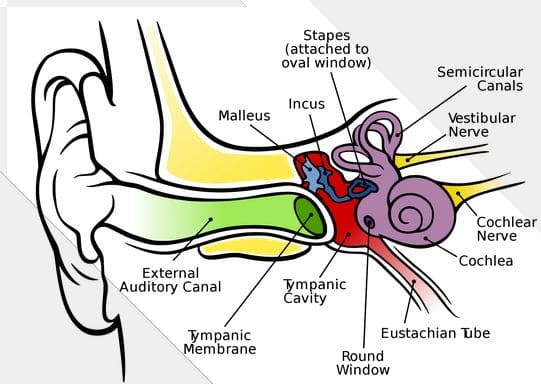
*Image courtesy wikipedia



