

The concept of Motivational Interviewing (MI) was developed by clinical psychologists William R. Miller and Stephen Rollnick to address treatment of problem drinkers (Miller & Rollnick 1991). Over the last several years there have been a number of articles in the audiology literature about how the principles of MI might be applied to the counseling of hearing aid candidates (Harvey 2003; Draper & Goyne 2017, even the latest 20Q at Audiology Online, written by Dave Citron). So, you might ask, what does the one (problem drinking) have to do with the other (hearing aid use)? My patients are not addicts!
It turns out that it is all about ambivalence.
About 3 years ago, after having read an article by Brian Taylor on Audiology Online concerning MI as a counseling tool (Taylor 2014), I was inspired to investigate MI more thoroughly by signing up for a 2-day seminar run by Stephen R. Andrew, a Licensed Clinical Social Worker and “Chief Energizing Officer” of the Health Education and Training Institute in Portland, ME. Of the 20 or so participants, I was the only one who was not a mental health professional. It was a powerful and revelatory experience. I was asked on more than one occasion what a hearing guy was doing at that seminar.
In psychological terms, ambivalence is defined as a state of uncertainty and fluctuation. It is wanting to do two different things or feeling two opposing ways simultaneously. In ambivalence there are conflicting feelings regarding the merits of change. Most of us experience this kind of ambivalence about something.
“I know I should floss my teeth more often. The dentist says it is good for my teeth and gums and I probably wouldn’t have so many dental problems and my teeth would look better. But it’s such a pain. It hurts my gums and I don’t like the way it feels. My teeth are pretty much OK as is anyway.” OR
“I know I should lose weight. I would feel better about myself. I would just feel better in general and I would fit into the clothes I really like to wear. But I just can’t seem to control it. Desserts always get the best of me. And it takes so long – I just don’t have the patience for it.”
The ambivalent person entertains conflicting and diametrically opposed feelings about the issue – whether to change or to maintain the status quo. Typically, status quo wins out. Does this scenario sound familiar in your clinical practice? The patient in denial about their hearing loss lives in a world of ambivalence.
When engaging with a person displaying ambivalence, the natural inclination is to try to confront arguments they are making for the status quo.
“It doesn’t hurt that bad. Your teeth are in pretty poor shape so you’d better do something!
You have more self-control than you think. Desserts are bad for you. Yes, it takes a while, but once you get going it gets a lot easier.”
MI, on the other hand, suggests supporting and bolstering the patient’s inherent willingness to change.
“Finally doing something positive about your teeth would relieve a lot of anxiety, don’t you think?
Yes, losing weight would improve your self-esteem; wouldn’t that feel a lot better? It would be nice to wear a wardrobe that you enjoy wearing, wouldn’t it?”
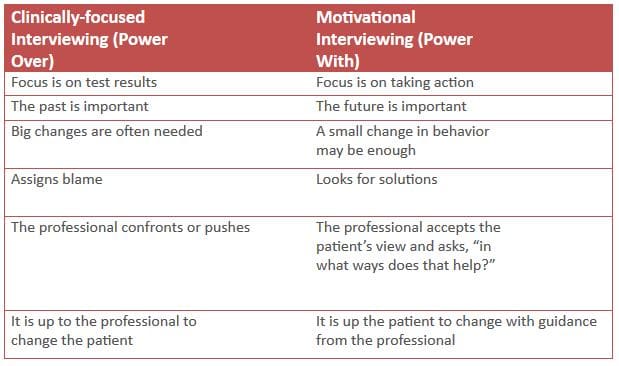
Most hearing care providers have been trained in a clinical or pathology-based, rather than a motivational or solution-based interviewing style. The clinical approach is characterized by an assess/diagnose/treat process. This approach views hearing loss as an impairment with a specific cause and effect for which the professional must find a cure or remedy. The attitude is, “The doctor knows best”, which leads to the “righting reflex”, where the problem is labeled and a quick fix is offered. This, in turn, is seen by the patient as a blow to their autonomy, to which their natural response is resistance (“You need hearing aids!” – “Oh no, I don’t!”) This approach may be effective when the patient presents with an ear pathology requiring medical intervention. However, when confronted with a patient’s ambivalence over a chronic problem such as sensory hearing loss, this clinical approach is much less effective.
Motivational Interviewing asks the hearing care professional to engage the patient’s own motivation for change, not by waiting for it to occur, but by offering compassion and deeper engagement. This is accomplished by understanding and exploring the patient’s own motivations, listening with empathy, empowering the patient, encouraging optimism and hope. We elicit the patient’s experience and perspective rather than impart
directives from a clinical mountaintop, thereby moving the patient from ambivalence to action.
Motivational Interviewing technique is characterized by the following principles:
- Avoid the “righting reflex”. (“This is the problem and here is how we are going to fix it.”)
- Compassion – (“I understand what you are going through”.)
- Ask open-ended questions and then listen deeply to the stories your patients tell, rather than looking for opportunities to talk yourself.
- Concentrate on identifying solutions to everyday communication problems, rather than the dwelling on the cause of the patient’s hearing loss or the results of the hearing assessment.
- Keep in mind that it is not the problem but the patient’s motivation that is the issue.
- Employ active listening. Reflect to the patient what they have said and then probe more deeply.
- Affirm the patient’s strengths and positive choices, rather than focusing on their shortcomings. This builds an atmosphere of trust and collaboration where the patient feels in control.
- Reinforce “change talk” – phrases that indicate a willingness to change, such as “I can…”, “I have to…”, “I will…”, “I’m prepared to…”, etc.
- Employ hypotheticals that give the patient a hopeful vision of the future. (“Imagine what it will be like when your family is not frustrated with your inability to participate in conversations at the dinner table. What would that be like for you?”)
“Status quo talk” – phrases that indicate resistance to change – if not completely ignored, should be engaged minimally. It is best not to contradict or argue with “status quo talk”. Rather, respond with questions that elicit “change talk”. (“Others certainly think you have a problem with your hearing. What do you think about that?” or “People are probably not going to speak any more clearly, so what can you do?”). Always reflect and reinforce “change talk”. (“So you do believe that doing something about your hearing would improve your relationship with your spouse.” Or “It’s a very insightful notion that improving your hearing could help bring you out of your shell.”)
For many hearing professionals, applying the principles of MI will involve rethinking years of training and experience using a clinically-based approach to counseling hearing aid patients. At the Maine seminar, I watched as mental health professionals struggled with an approach that upends many long-held tenets of psychological counseling. I hope you may be encouraged to attempt this method, and to persevere. It may be a bit uncomfortable at first – not unlike holding a golf club or a musical instrument correctly for the first time. My first time using this approach with a patient was a bit awkward and I was tempted to abandon the experiment. It quickly became more comfortable, particularly as I experienced positive results. I am confident it will be the same for you.
References:
Draper E, Goyne TR (2017). Motivational interviewing: An introduction for audiologists. Audiology Today, Sept/Oct: 29:5, 26-33.
Harvey, MA (2003). Audiology and motivational interviewing: A psychologist’s perspective. Audiology Online, Article 1119. Retrieved from: https://www.audiologyonline.com
Miller WR, Rollnick S (1991). Motivational interviewing: Preparing people for change. New York: Guilford Press.
Taylor, B (2014). Keys to in-clinic success: Introduction to solution-focused interviewing. Audiology Online, Course #25576. Retrieved from: https://www.audiologyonline.com
*featured image courtesy flckr
 Paul U. Teie, MS, is a national sales trainer for HearUSA and HearCanada. He can be reached at [email protected]
Paul U. Teie, MS, is a national sales trainer for HearUSA and HearCanada. He can be reached at [email protected]




