

Last week, Paul Teie was a featured guest blogger at Innovations in Hearing Heathcare. This week, Paul joins his colleague, Cecelia Wickert, to share their thoughts on the subject of patient denial and how this common behavior affects treatment decisions.
This patient is “in denial”! We all know what that implies. The patient is blaming others for the hearing difficulties that we and those closest to them know originate with them. He (or she – this is not a gender-specific state) is being stubborn, unreasonable, resistant, and downright bull-headed when it comes to doing something about their hearing loss. It is a common condition and is not at all unexpected. All hearing professionals are well aware of the oft-repeated statistic saying that the average person with hearing loss is conscious of the situation for 5 to 7 years before doing anything about it.
Assuming this is true (and there has been nothing in our experience to doubt it), experience also shows that denial is not a single state of affairs. There are degrees and shades of denial that can be described as a continuum that commences with absolute denial and, it is hoped, culminates in acceptance.
The “seven-year stretch” must not be accepted as a given. At each point in the continuum of denial, hearing professionals have an opportunity to move their patient forward, ever closer to acceptance of their hearing loss and the help we can provide. An effective way to accomplish this is to identify the patient’s ambivalence (that is, their internally warring notions that change is a positive thing but that the status quo is preferred), and to cultivate the patient’s desire for change rather than to focus on contradicting arguments for the status quo.
In nearly all the 6 levels of denial that we have identified (not unlike the Kübler-Ross Stages of Grief), embedded within the expression of denial is some degree of acknowledgement that change is desirable.
The Continuum of Denial
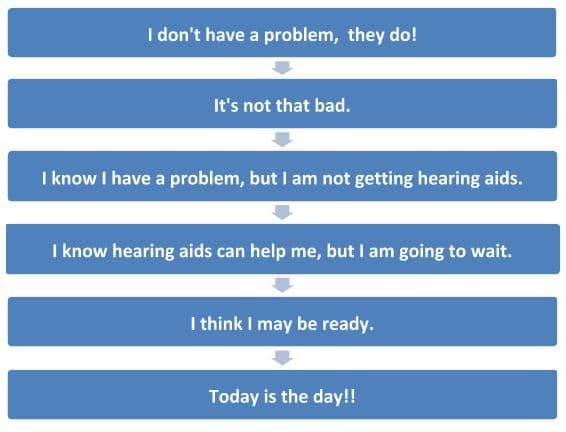
Level 1 – I don’t have a problem, they do!
At this stage, there is little or no acknowledgement that any change is required, much less desirable. Only further probing is likely to shake the foundations of this patient’s conviction that they are being sold a bill of goods. “Your family seems pretty convinced that you have a hearing problem. What do you think about that?” Or “It’s pretty unlikely that everyone you meet will simply start speaking more clearly, so what do you think you can do?” Questions such as this may serve to, at the very least, plant some doubt in the mind of the patient in denial that others are the sole source of their difficulty. This can begin moving the patient toward acceptance.
Level 2 – It’s not that bad.
Suggested in this brief sentence is the beginning of acceptance. What is implied in this statement is, 1) I have hearing loss, 2) it is noticeable, 3) if it were any worse, I would maybe think about doing something about it. Our natural inclination in response to a patient at this level of denial is to counter, “Yes, it is that bad! Look at this audiogram, why don’t you! See how far down the graph the X’s and O’s are?” A better approach would be to explore the three implications: “So you do think you have hearing loss. In what kind of situations has it been noticeable? Tell me how that has made you feel? How bad will it have to become before you would be willing to do something about it?”
If it has not already come up, now might be a good time to educate your patient regarding the consequences of untreated hearing loss. (I suggest these consequences may be better mentioned earlier, when describing the patient’s hearing loss. When presented at this point in the process it may well be seen as a “sales tactic” and the provider’s credibility could suffer. When addressed, with all patients, earlier in the process, it will be recognized as intended, as education.)
Level 3 – I know I have a problem, but there is no way I am getting hearing aids.
At this stage there is definite acknowledgement of a hearing problem. The problem now is the hearing aids. First, elicit more detail regarding the acknowledgement: “What kinds of problems do you see yourself having with your hearing? What are those around you saying to you about your hearing? What do you think you can do about these problems now? What value might there be in overcoming these problems?” Then address the issue of hearing aids. “What is it that you believe hearing aids do? How do you imagine hearing aids might be helpful in those situations? Do you have any friends or family that have found hearing aids helpful? What do they say about them?” The HCP should take this opportunity to dispel, in a non-defensive, non-confrontational and positive way, any misconceptions your patient may have regarding amplification. This can include descriptions of success stories from your experience.
Use of the feel-felt-found formulation can be helpful:
- I understand how you feel. (Conveys empathy)
- I have had many patients (be as specific as you can be, ethically) that have felt that way. (You are not alone)
- But most of them have found a) that not to be the case (or) b) that hearing aids have been very helpful in that kind of situation. (Hearing instruments are effective)
Level 4 – I know hearing aids can help me, but I am going to wait.
This is the first indication of an acknowledgement by your patient that hearing aids may be in their future. Questions regarding hearing aids can now be couched in more unconditional, less hypothetical terms (will vs. would – do vs. may, etc.): “How do you see hearing aids improving your life? What kinds of situations do you think hearing aids could help you? How will your family and friends respond to your hearing better and being able to fully take part in activities with them?” Then address the issue of putting off an investment in hearing instruments. “How do you see waiting to get help with your hearing as being beneficial to you or to your family? How long do you think would be an optimal length of time to wait?” Again, reinforcing the consequences of untreated hearing loss may be indicated.
Level 5 – I think I may be ready.
At this point in the process there is much that is positive to reinforce. By helping your patient to verbalize (and thus, “make real”) that which they have up to now only been thinking, it should be a simple matter to help them come to the realization that today is the day for them to make this important decision. We can do this by encouraging our patient to verbalize what they believe hearing aids will do for them, the benefit hearing aids will provide for their loved ones, and why it is no longer desirable to wait. When the patient does not verbalize these things themselves, we can offer them a vision of hope in a future with hearing instruments: “Just think how great it will be for you to be able to understand your grandchildren. How do you think your wife will respond when you are able to fully take part in family activities? You can leave today with better hearing! Isn’t that exciting?”
Level 6 – Today is the day!
Acceptance!! Cue the Hallelujah Chorus! For the moment, we are finished asking questions. Rather, reassure your patient they have made a positive choice for themselves and their family and promise to be at their side throughout the upcoming process.
Not all our patients need be doomed to endure the forecast 7 years from when they realize they have a hearing problem to making the decision to do something about it. By understanding where along this continuum of denial our patient stands, we have an opportunity to ask questions that tap into their willingness to move forward. By so doing we may be able to help them to move from “I don’t have a problem!” to “Today is the day!” in a much shorter period.
Cecelia Wickert and Paul Teie are National Sales Trainers for HearUSA/HearCanada
*featured image courtesy flckr



