
Editor’s Note: Providing adequate clinical education in audiology has always been a challenge for most university programs, but this has become especially true over the past year in the midst of a global health pandemic. This week, HHTM President and CEO, Kevin Liebe, interviews Robert Koch, President and founder of AHead Simulations, on how his company is helping to address gaps in clinical education in hearing healthcare.
KL: Can you provide us some background on how your company got started? What drew your interest to simulators?

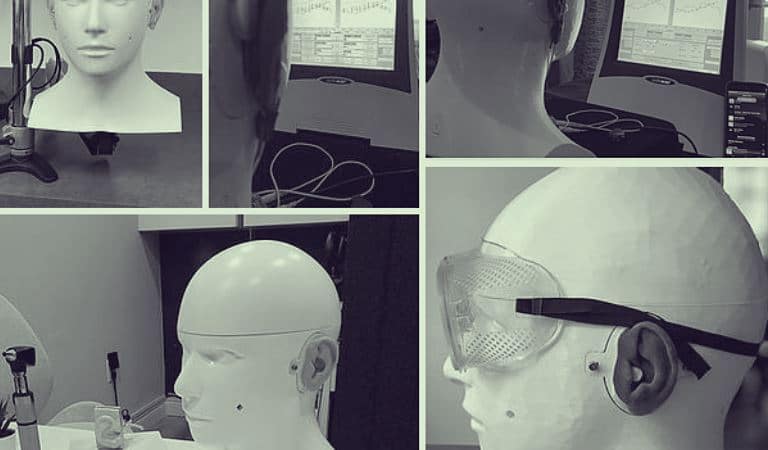
CARL
RK: To be honest, it wasn’t so much an interest in simulators, as much as an interest in the hearing healthcare field! Back in 2015, I was in my 4th year of electrical engineering at Western University and I was connected with the amazing people at the National Centre for Audiology in Canada, including Dr. Susan Scollie & Dr. Paula Folkeard. They had recognized at the time that the way they were teaching their students had room for improvement – they didn’t have enough hands-on training opportunities in their classroom outside of practicing with each other/volunteers.
At Western University, there’s a heavy focus on the medical field, and other departments such as Nursing and their School of Medicine used medical simulation in almost everything they do, so it seemed out of place that the Department of Audiology had little simulation equipment of their own.
To address this training gap, we started to put together our version of a manikin meant to simulate a hearing loss patient with an overarching goal to get training within hearing one step closer to these other medical disciplines. Our starting point was developing a simulation for probe tube placement, and it only grew from there (read about the background on CARL here).
Almost 6 years later, there are over 100 CARLs in use around the world for not only real-ear measurement, but for cerumen management, earmold impressions, on-head & on-ear fitting, and anything else which may typically be done on a patient/volunteer.
KL: Most hearing professionals have worked with simulators of some kind during their training – what makes AHead unique?
RK: One thing that makes AHead unique is that we came directly out of a need. AHead wouldn’t exist if there wasn’t a gap within training. There are simulators for specific tasks/procedures, foam heads and ears that can be custom-made by programs, or extremely expensive equipment like KEMAR, but none of these are a ‘one-stop-shop’ for training all the core procedures and competencies within hearing healthcare. With CARL, we wanted to have a platform in which the core manikin simulates a hearing loss patient in as simple a way as possible. You can use any equipment, any hearing aids, and any training material you want with CARL. If you want the additional camera capabilities within CARL (seeing real-time video of what’s happening within CARL’s ear canal), then that could be an option as well, but the base of CARL is a consistent, high quality manikin for all of your hearing healthcare training.
Something that has been extremely important for us is that CARL is routed in rigorous simulator validation to ensure what we’re producing has been proven to show an impact on clinician competency. By maintaining a strong relationship with the research and clinical community, we can make sure that our products are having a day-to-day impact on the trainees, trainers, and ultimately the clinical practice that patients will experience.
I would say we are also unique in the way that we produce and develop CARL at AHead. 3D printing isn’t new to the audiology field with earmolds and shells regularly produced that way, but we are taking it a step further and using the latest 3D printing technology and techniques to bring CARL to life (literally!). We develop and produce everything in-house meaning that every single CARL leaving our doors is better than the last. We also have CARL built as a modular platform so that any new modules or any new ear anatomies that we come out with can work with an existing CARL out there! This allows us to continue iterating CARL as fast as we can to quite literally become your “Perfect Patient”.
KL: Receiving adequate clinic education during a pandemic has been a major challenge for many audiology programs. Did you see a lot of programs switching to use simulators like AHead?
RK: We did see a considerable interest in simulation during the pandemic and during the switch to online training. As with any change across the industry, the pandemic was an extra ‘push” showing that the way things have always been (practicing and gaining experience on live patients only) just isn’t sustainable and not practical as the industry and the world changes and evolves. Simulation has several benefits, and I think the key benefit to facilitating training while social distancing, or even remote-training with CARL on one side of the video, and the instructor on the other, has really shown itself this year.
What we see as common with adopting simulation is that there’s a barrier to getting that first implementation or first use case. It takes a big paradigm shift to see training in the light of simulation and do things in a completely different way with new equipment – it’s not easy! That first use case (whether it’s earmold impressions, real-ear, or cerumen management) is always tough to implement, but once it’s successful and they realize the benefits of this new paradigm, the barrier for implementation becomes lower and lower, and eventually you could never picture yourself going back to not using simulation.
If you ask current students within hearing healthcare that have used simulation during their entire education, it is very difficult for them to imagine what that education would have been like without the use of simulation. I think the extra emphasis on simulation that the pandemic has created will initiate a change that will continue to be seen in the years ahead.
Lastly, I think it has opened people’s perspective to what simulation is all about. Simulation doesn’t only mean using a manikin, or using a piece of software. Simulation is about experiential learning – simulating experiences, simulating procedures, simulating patients, simulating environments. It’s all about doing things better by rehearsing first – and I truly believe it’s as much a mindset as it is a technology adoption with simulators like CARL.
KL: Where can people go to learn more about CARL and what you’re doing at AHead Simulations?
 Robert Koch is the President and Founder of AHead Simulations, a hearing healthcare startup in Ontario Canada guided around improving the quality of hearing care through advanced simulations. Robert began his work on CARL in 2015 at Western University, and commercialized the CARL Simulator while receiving his Master’s of Biomedical Engineering.
Robert Koch is the President and Founder of AHead Simulations, a hearing healthcare startup in Ontario Canada guided around improving the quality of hearing care through advanced simulations. Robert began his work on CARL in 2015 at Western University, and commercialized the CARL Simulator while receiving his Master’s of Biomedical Engineering. Kevin Liebe, AuD, is President and CEO of Hearing Health & Technology Matters (HHTM). He also serves as a Scientific Advisor to Neosensory, a Silicon Valley based startup pioneering experiences in sensory augmentation. As an audiologist, Kevin has experience in variety of settings, including private practice, ENT, and industry. He is a past president and board member of the Washington State Academy of Audiology
Kevin Liebe, AuD, is President and CEO of Hearing Health & Technology Matters (HHTM). He also serves as a Scientific Advisor to Neosensory, a Silicon Valley based startup pioneering experiences in sensory augmentation. As an audiologist, Kevin has experience in variety of settings, including private practice, ENT, and industry. He is a past president and board member of the Washington State Academy of Audiology

