
HHTM staff
Today’s post continues the discussion of Hansen’s disease, commonly known as leprosy, as part of HHTM’s series on insidious, successful diseases of long-standing that may have effects on hearing and balance.
Gaining information on such diseases is the first step that Audiologists and other health professionals need to take in order to recognize and handle rare sightings and their effects. Today’s post is a basic primer on the disease known as leprosy and properly called Hansen’s disease.
Recap from Last Week
Hansen’s disease is caused by secretive bacteria that lead a successfully hidden, parasitic lifestyle in humans. It’s also sneaky, masquerading as a variety of human ailments and resolutely dying off in lab cultures, which has led to scientists doing crazy things to try to “capture” it in action (Launer, 2007). The disease is hard to diagnose clinically and the parasitic bacteria is hard to study scientifically.
The effects of leprosy on the ear and hearing are not well known but we do known they exist. Likewise, the presence of leprosy is not well known in the US, even though 100-200 new cases are found each year. The World Health Organization (WHO) characterizes leprosy as a “neglected” but eradicable disease that has low mortality figures but a heavy toll on healthy years of life. That number is likely to increase as global travel increases to “exotic” locations where the disease is common and hundreds of thousands of new cases are found annually.
How Do You Get Leprosy?
Not surprisingly, this is the first question people ask when the subject of leprosy comes up. Surprisingly and alarmingly, there’s not a clear answer. Difficult as it is to believe in this day and age, leprosy’s transmission mode is unknown.
It’s hypothesized that the bacillus invades its host (usually, that’s us) through the skin or via the upper respiratory tract (Chow & Roman, 2008). Direct touch by an infected person was thought to be the mode of transmissions for centuries, hence the creation of leprosy colonies to isolate those with the disease. More recently, the upper respiratory tract has emerged as the most likely route, based on experimental data in mice (Shepard, 1960). If that’s so, then leprosy is most likely spread by nasal droplets spread airborne communication from person to person, similar to tuberculosis.
However, the possibility of transmission through insects, similar to malarial and Lyme disease infection, remains a possibility which has not been completely ruled out
Who Gets Leprosy?

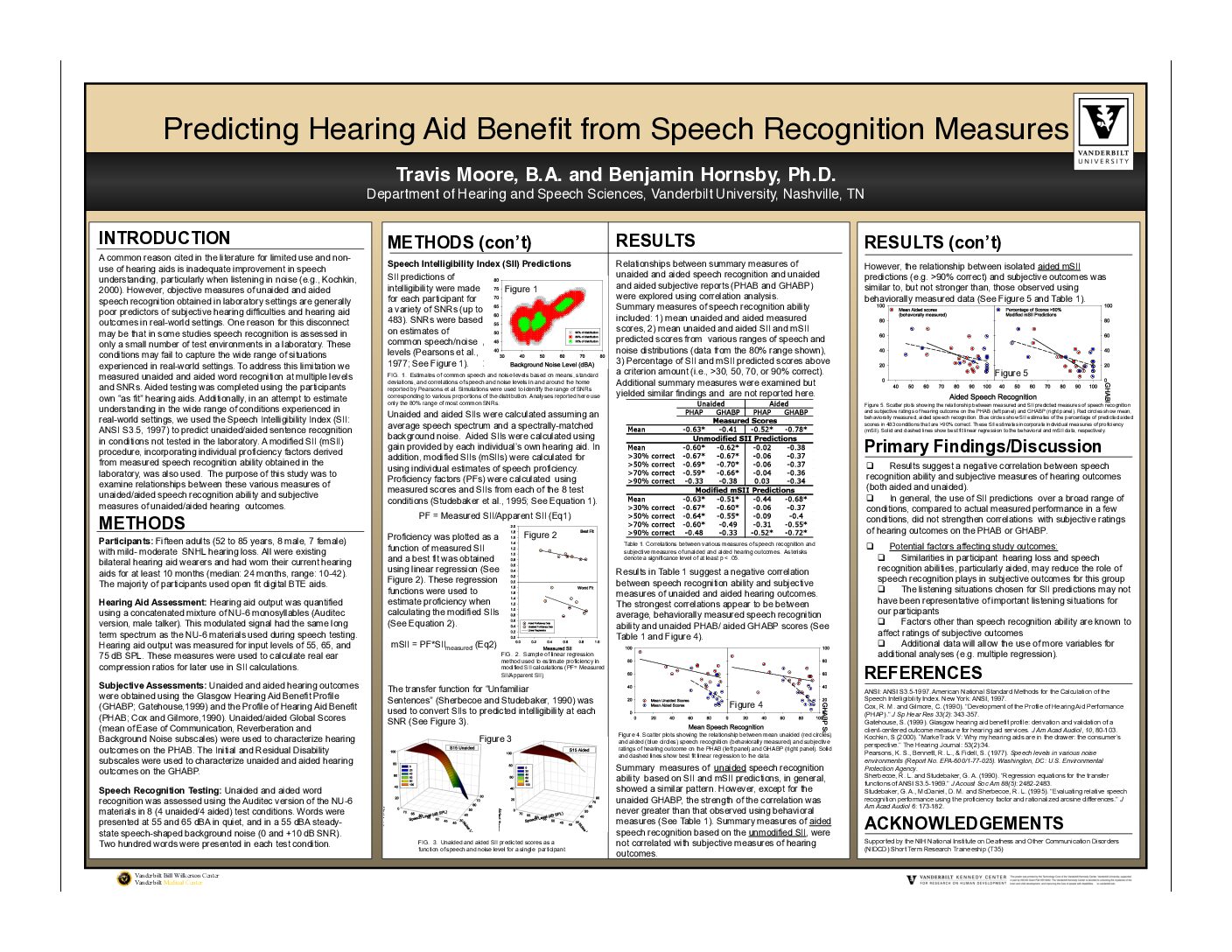
Figure 1. Distribution of leprosy by country.
The good news is that leprosy is not easy to get. First, it can only be spread by those who have the disease but have not been treated (yes, there’s a treatment). Second, most people appear to be resistant to leprosy, either not getting it at all or getting a negligible infection that does not persist in their bodies (Werner, 2009). The latter are said to be “cured spontaneously.”
The bad news is that an estimate 5 percent of people lack immunity, due to a cellular defect in their DNA. Interestingly (but maybe not related), the defective DNA region is the same one associated with Parkinson’s disease (Buschman & Skamene 2004).
Leprosy is not age specific. According to the WHO, it occurs in humans from early infancy to very old age. The same WHO report states that males get it more often than females by a ratio of 2:1 in most parts of the world, but a few geographic areas (especially in Africa) have equal representation by gender or have a somewhat higher ratio for females.
Leprosy is endemic throughout the world but is more prevalent in developing countries (Fig 1). Note, however, that gray areas of the WHO map in Fig 1 do not denote absence of leprosy; rather they denote “not measured,” consistent with the WHO’s own designation of Hansen’s as a “neglected” disease. Absence of data underscores the fact that cases in the US are often diagnosis with much delay, in part because physicians are not aware of the possibility of leprosy and its symptoms, in part because it is not a disease for which data is collected in developed countries.
Geographic differences do exist for different types of leprosy. One severe type (diffuse lepromatous leprosy) occurs mainly in the Carribean and Mexico where it has been endemic for many years. It has now been tracked to previously unknown leprosy virus (M. lepromatosis) with a slight but significantly different RNA gene “fingerprint” (Han et al., 2008).
What’s Next
Next posts will go into what happens when the bacillus invades, how it creates nodules, how it attacks the outer ear (see feature picture in the title), and what effects are known to occur in the auditory and vestibular systems. Eventually, there will be a discussion of treatment and what, if any, effects it has on hearing aid vestibular disabilities caused by the disease.
Feature Image courtesy of Wikimedia


