
This is the next chapter in a multi-part Shingles series originally prompted by an obscure link to Red Ear Syndrome. That link lead to posts on shingles in general, shingles in the ear, and the specifically-named Ramsay-Hunt Syndrome Type 2 (RHS/2) .
RHS/2 is a horribly painful condition in which the herpes zoster in the geniculate ganglion reactivates and manifests in any number of ways, including deafness, vertigo, pain, and facial weakness/paralysis. RHS/2 is difficult to diagnose and distinguish from other problems. For example, it is almost always characterized by a severe rash but it can also occur with facial paralysis without a rash, similar to Bell’s palsy and that’s what today’s post is about.
What’s an Erythematous Vesicular Rash? What Does it Mean?
This rash is like Supreme Court Justice Potter Stewart’s famous definition of obscenity–you know it when you see it. In this case, you definitely know it when you feel it because of the extreme pain. Erythematous vesicular rash affects skin as well as mucous membranes, such as the lining of the mouth. It is characterized by
“large, symmetrical red blotches [which] appear all over the skin in a circular pattern. On mucous membranes, it begins as blisters and progresses to ulcers.”
The problem with this rash is that it can be caused by a variety of things (e.g., medications) that have nothing to do with Ramsay Hunt or infection of any kind. For example, it can be misdiagnosed as a kissing bug bite (which raises the spectre of Chagas disease), based on the presence of vesicular rash by the lip. Even more of a problem is that RHS/2 can occur without any rash anywhere, a situation referred to as “sine herpete” in the medical literature.
The presence or absence of facial erythematous vesicular rash is not diagnostic for RHS/2, though its presence surely should gain the attention of the physician and its absence in the presence of facial paralysis should not rule out RHS/2.
All in the (Herpes) Family
We’ve tried to make this series clear and simple, but the anatomy and physiology have defeated our efforts. Just talking about the geniculate ganglion takes us places we never went in hearing and speech anatomy classes. The varicella zoster virus (VZV) and its cousin herpes simplex virus (HSV) are better versed in the anatomical pathways than we are. Once unleashed, they seem to ride those pathways like highways, taking little-known, interconnected neural shortcuts as they please. Pulling it all together, as best we can, here’s a brief summary of what the zosters can get up to:
- HZ oticus. Just the ear. Caused by VZV in the geniculate ganglion. Herpes zoster oticus affects any/all parts of the peripheral ear: external (pinna, ear canal, eardrum), middle, and inner (cochlea). It causes severe ear pain associated with vesicular rash. Hearing loss, if present, varies in severity and permanence.
- RHS/2. The ear and the face. Caused by VZV in the geniulate ganglion. When HZ oticus is accompanied by facial paralysis, it becomes Ramsay Hunt syndrome. Just to confuse things, we noted in our last post on this subject that strictly speaking, you can have RHS/2 without any signs in the ear, in which case it’s RHS/2 without herpes zoster oticus. Confusing. But most of the time the ear’s involved so herpes zoster oticus is frequently referred to simply as Ramsay-Hunt.
- RHS/2 sine herpete. The ear and the face, but no rash. This is confusing. There is no rash (sine herpete) but there is facial paralysis and other symptoms, some involving the ear. Caused by VZV in the geniculate ganglion.
- Bell’s palsy (also called Bell palsy). Facial paralysis/weakness, no rash. Unlike HZ oticus and Ramsay-Hunt, Bell’s palsy is thought to be caused by herpes simplex virus (HSV) type I infection in the geniculate ganglion, NOT by VZV. Bell’s palsy is staged according to degree of facial weakness from Stage I (normal facial function) to Stage VI (total single-sided facial paralysis).Facial paralysis in RHS/2 may be more severe and lasting than that of Bell’s palsy, though that probably depends on the Stage of Bell’s palsy. You can imagine, though, that RHS/2 sine herpete and Bell’s palsy are easily confused — both show facial paralysis/weakness, neither shows a rash. And just to confuse things even more, Bell’s palsy can paralyze the muscles of the middle ear, effecting the same result as some forms of HZ oticus. Blood tests can distinguish which virus (VZV or HSV) is present.
The bottom line for audiologists is that a complete audiometric workup is necessary for patients who present initially or upon return, with complaints of sudden-onset unilateral ear pain, hearing loss, dizziness, facial paresis or rash. As soon as testing is completed, send the patient–audiogram in hand–for ASAP workup by their physician or an ENT, with the goal of arriving at a diagnosis and treatment as quickly as possible. In many cases, early treatment can mitigate symptoms and reduce long-term effects.
What diagnoses are made or ruled out when patients are worked up medically? We’ll look at some case histories and competing diagnoses when we next write about Shingles in this series.
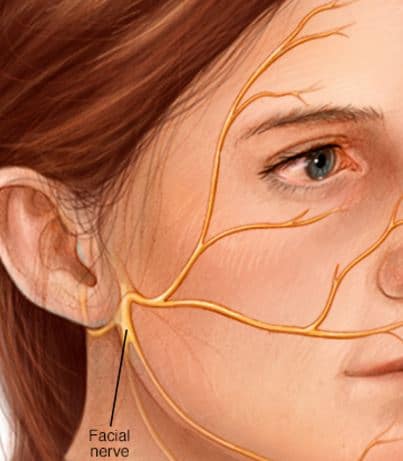
feature image from Mayo Clinic



Excellent article! As typical of many of us, I was misdiagnosed as cellulitis and Bell’s Palsy in 2008. I was prescribed the BP dose of antivirals, which are/were one fourth the strength of RHS. Months later a MRI showed an active lesion. CN VII on the RHS side. Zoster was still munching away at my nerves, doing damage, which nine years later is still disabling. Articles like this one, full of important, realistic and easy to understand information need to be widely distributed to educate as many people as possible. RHS can be such a horrid disease. Accurate and fast treatment is imperative.
August 13, 2017
Hello from Iowa…Very informative article….Thank you..
I have been to 3 general doctors and two ENT doctors since onset in January.
I was given antibiotics from January thr March…then Valacyclovir in May.
I joined the Ramsey Hunt Sndrome Group on facebook and someone shared your wonderful article.
My symptoms have been all around the left ear..inside and out..dizziness, nausea, and exgtreme tiredness.
I no longer have the sores..but have painful post therapic neuralgia in the bowl of the ear.
My doctors have had a tough time working with my illness…as the general pracitioners never see this…and the ENTs rarely.
From reading your article I believe I have the HZ oticus as I do not have any facial problems. I would love to hear responses as to how I might get over the PTN and tingling sensation that I have along the nerve lines. My ENT suggested I have an MRI..should I ?? Thank you so much.