
Shingles in and around the ear and face is awful. This post series has belabored the pain and agony problem enough. The other big problem, the subject of this final post on the topic, is that it’s often very hard to diagnose and differentiate from other disease processes, especially in older patients. Here’s where the last post left off:
… do complete audiometric workups on patients who present initially, or return, with complaints of sudden-onset unilateral ear pain, hearing loss, dizziness, facial paresis or rash. As soon as testing is completed, send the patient–audiogram in hand–for ASAP workup by their physician or an ENT, with the goal of arriving at a diagnosis and treatment as quickly as possible. In many cases, early treatment can mitigate symptoms and reduce long-term effects. What diagnoses are made or ruled out when patients are worked up medically? We’ll look at some case histories and competing diagnoses when we next write about shingles in this series.
What to Look For and What to Make of It
Misdiagnosis of shingles hinders treatment and predictive outcomes. Audiologists do not make the diagnoses or prescribe the treatments but they should know what to look for and how/when to refer when working with patients who present with a variety of symptoms or complaints. They should also know the complications of shingles, which can affect hearing and auditory function.
Table 1 lists symptoms manifest in shingles which are easily confused with other problems and diseases.
|
Shingles Presenting Symptom |
|
| Pain/swelling in ear canal | External otitis |
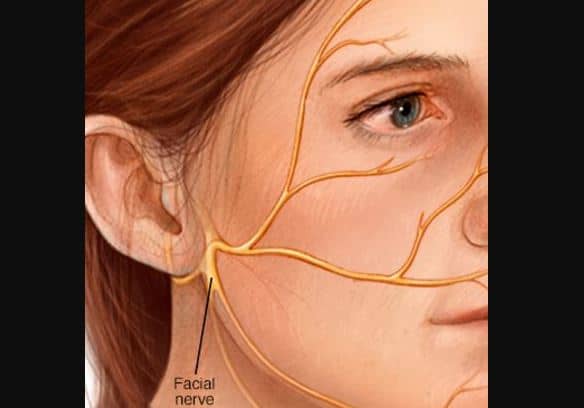
| Unilateral facial weakness | Bell’s palsy |
| Vertigo |
Viral labyrinthitis Stroke, posterior inferior cerebellar artery (PICA) region |
| Paroxysmal pain precipitated by cold wind, face washing, etc. | Trigeminal neuralgia |
| Facial pain and/or ear pain |
TMJ Dental abscess Nasopharyngeal carcinoma Otitis media |
Shingles Complications
We’re not going to list everything — you can imagine where varicella can take you… and leave you, but here are the two ends of the spectrum:
- The most common complication is post-herpetic neuralgia — pain and itching remain after shingles rash/blisters resolve. There is no cure treatment for this condition.
- A very rare complication is encephalitis. Thankfully, this life-threatening inflammation around the brain takes a mild form in the case of herpes zoster and reportedly resolves quickly, except in patients with impaired immune systems, when it can be deadly.
A Shingles Case History
Finally, for those audiologists or others who have some degree of comfort looking at brain scans, click on the link for an interesting one showing a case history of Ramsay Hunt at work in the inner ear, cranial nerves, with neural degeneration extending into the brainstem. This was a 58 year old man who presented with extreme ear canal pain with vesicles, complete unilateral facial palsy,severe hearing loss, and vertigo for 28 hours. Ramsay-Hunt was confirmed by blood serum and contrast MRI was performed on the 3rd day post-onset.
He was treated with IVAcyclovir and corticosteroids, together with pain medication. At hospital discharge 8 days later, he had “partial recovery” of hearing loss and facial paralysis. Considering what he’d been through, it is perhaps not surprising that he refused to return for repeat MRI or other tests, so the extent of permanent hearing loss or neuronal degeneration in the auditory system is unknown.
Treatment
(Note: Information in this section is from a single source: patient.co.uk)
Antiviral drugs approved for shingles include: acyclovir (Zovirax), famciclovir (Famvir), and valacyclovir (Valtrex). These drugs are supposed to be prescribed no later than the first week after shingles onset, which is a challenge if the condition is misdiagnosed.
If treatment goes into effect in the first three days, about 75% of people achieve full recovery from shingles, although the effects of treatment for Ramsay-Hunt variety are not as clear cut. Hearing loss reportedly resolves but facial paresis may persist in those who do not fully recover. In general, aging, diabetes, and high blood pressure are additional risks for full recovery.
In addition to anti-viral treatment, prednisone in combination with acyclovir has been shown to reduce facial paralysis but prednisone has no effect on recovery of hearing loss.
Diazepam is sometimes used for vertigo.
Vaccination
Zostovax is available for those 50 and over who have already had chicken pox. The vaccine is a weakened form of the varicella-zoster virus. It reduces the risk of shingles by about 50%, may reduce the likelihood of recurrence if you’ve already had it, and shortens the period of post-herpetic neuralgia. It’s not for everyone — people with histories of HIV, leukemia, cancer treatment shouldn’t take it; pregnant women shouldn’t. These and other contra-indications are checked before you can get the vaccination.
A small group of people never develop immunity to the varicella virus, either because they didn’t get chicken pox or they didn’t get the chicken pox vaccine. Tthose people are not at risk for shingles, but they are at risk for severe infections if they are eventually exposed to the virus. In people with compromised automimmune systems, such exposure can prove fatal. A new drug has just been approved to provide some relief to those people if they develop chicken pox. Looked at from this perspective, perhaps shingles is not so bad after all….. just ask Barbara Walters, a victim of chicken pox at 83 which was delayed in diagnosis after she suffered a fall and developed persistent fever.
Enough about shingles! We’re on to other, less painful topics in future posts. Thanks for reading this series and we hope it has been helpful to our readers.



I have been reading about this medical condition these days and there are many people who are still unaware of the symptoms and the treatments available.