

Last August, a post in this section described unusual findings in a patient with unilateral sensorineural hearing loss and retrocochlear findings who was referred for MRI to rule out acoustic neuroma. An acoustic neuroma is a benign, small, slow-growing tumor on the VIII cranial nerve–technically called a vestibular schwannoma.
The MRI found no evidence of a tumor but surprisingly identified a “vascular loop” occupying some of the space reserved for the VIII nerve to emerge from the inner ear and enter the brain. Vascular loops can mimic symptoms of acoustic neuroma and that’s the topic of today’s post.
What are Vascular Loops? How Does it Cause Hearing Loss?
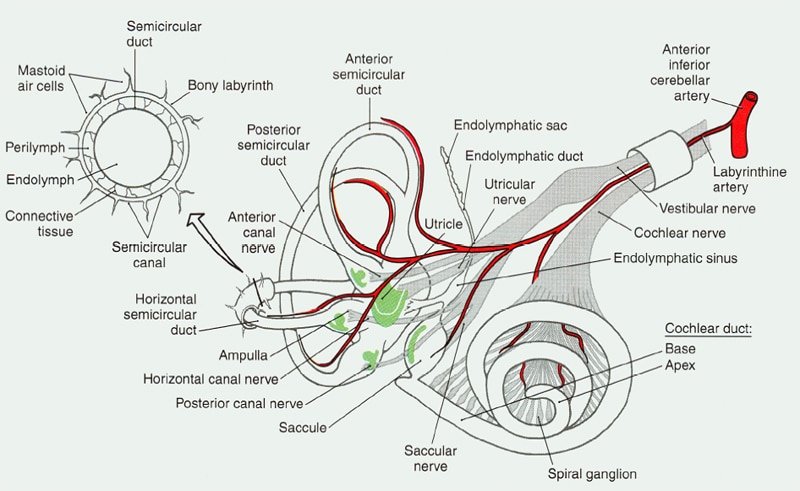
Figure 1. Blood supply to peripheral auditory-vestibular system.
Vascular loops are anatomical anomalies of the anterior inferior cerebellar artery (AICA). We mention that artery because it is the blood supply for the inner ear, which includes hearing and vestibular (balance) systems. Figure 1 shows the system with the blood supply shown in red.
Notice how it “shares” a narrow passage way with the vestibular and acoustic branches of the VIII cranial nerve. Without the VIII nerve, we do not hear. The result is the same if the blood supply is compromised due to injury, space occupying lesion, disease, or anatomical anomaly.
A Bottleneck
In Figure 1, the artery and two nerve branches appear wrapped in a little cylinder. That’s just a visual so you can see how they lie inside the skull. In actuality, all three pass through a short (about 1 mm) narrow little corridor (about 3.5 mm) that nature drilled into the temporal bone before entering the brain proper in what’s called the cerebellopontine angle (CPA).
The connecting corridor — called the internal auditory meatus — protects the blood and nerve supplies while linking the ear and vestibular system to the brain. That doesn’t leave much room for error or extras. Speaking of extras, the facial nerve also goes through that corridor, though it’s not shown in figure 1. Talk about a traffic jam! No room left at all now.
The Traffic Jam: Injuries But No Fatalities
Yet, into this bottleneck extra vascular AICA anomalies in the CPA can nudge and impose, “suspected of causing hearing loss, tinnitus, and vertigo” due to “the complex interaction between the vascular loop and eighth cranial nerve, in which the loop exerts pressure on the nerve, and the nerve compromises inner ear circulation.”
One study looked at 15 patients with unilateral (one-sided) or asymmetrical hearing loss and/or tinnitus who had imaging of the CPA suspected acoustic neuroma but were found to have vascular loops instead. Complete audiovestibular work-ups on those patients revealed:
- the already-established hearing loss on the side with the vascular loop
- good, symmetrical, word recognition performance in both ears
- spontaneous nystagmus (a vestibular sign) in 14 of the 15 subjects
- a low proportion (one-third) of subjects with abnormal calorics (a test of the vestibular system)
- no significant relationship between presence of tinnitus and presence or position of vascular loops vis-a-vis the auditory portion of the VIII nerve
The auditory findings of this study agreed with previous research by McDermott et al (2003) who reported a “clear” relationship between vascular loops and unilateral hearing loss, but not with tinnitus, in a prospective imaging study of over 300 patients with complaints of unilateral hearing loss and/or other “auditory symptoms.”
From these studies and others, Applebaum and Valvasorri (1985) arrived at the follow recommendation for practitioners:
Eighth nerve tumors and vascular loops produce similar symptoms, but a cochlear type of hearing loss with good speech discrimination and normal caloric testing should raise suspicion of a vascular loop.
Despite the suggested profile of “good, symmetrical word recognition scores,” the patient in last August’s post presented with poor speech discrimination on the involved side and almost 20% roll-over. Even more reason to get an MRI. Other studies associate vascular loop with unilateral pulsatile tinnitus accompanying same-ear hearing loss (Ramly et al., 2014). See Chadha and Weiner (2008) for a review of studies.
According to the reports in the literature, as well as the recommendations given in the aforementioned case study, surgery is rarely recommended for AICA loops. From the patient’s perspective, this is a good news/bad news conclusion: there is no tumor, but no treatment for the permanent unilateral hearing loss.
References
Applebaum & Valvasorri. Internal auditory canal vascular loops: audiometric and vestibular system findings. Am J Otol. 1985 Nov;Suppl:110-3.
Chadha NK & Weiner GM. Vascular loops causing otological symptoms: a systematic review and meta-analysis. Clin Otolaryngol. 2008 Feb;33(1):5-11. doi: 10.1111/j.1749-4486.2007.01597.x.
McDermott et al. Anterior inferior cerebellar artery syndrome: fact or fiction. Clinical Otolaryngology & Allied Sciences. Volume 28, Issue 2, pages 75–80, April 2003.
Ramly NA et al. Vascular loop in the cerebellopontine angle causing pulsatile tinnitus and headache: a case report. EXCLI J. 2014; 13: 192–196. Published online 2014 Feb 27. PMCID: PMC4464511
images from athelonwealth & studyblue



