

 The six previous posts on the human ear canal focused primarily on its dimensions.
The six previous posts on the human ear canal focused primarily on its dimensions.
This post is directed toward non-dimensional features of the ear canal that lead to an understanding of the tissue, blood supply, and innervation of the ear canal.
Skin Lining and Substructure
The skin lining of the osseous (bony) canal is much thinner than that of the cartilaginous canal, measuring about 0.1 to 0.2 mm in thickness, and is continuous with the skin covering the lateral surface of the tympanic membrane and the auricle (Figure 1). As a result, no glands or hair follicles are found in the bony canal, and coupled with the thin tissue; there is little movement in this section of the canal.
In the bony auditory meatus, the skin is closely applied to the periosteum (Figure 2). This limits expansion in the event of inflammation, and accounts for the severity of pain so often encountered in meatus furunclulosis, or when objects come into contact with the bony canal wall. The thickness of the skin diminishes from without inwards, and in the deeper meatus is extremely thin and fragile. This predisposes this portion of the canal to trauma during manipulations as well, most often in the form of a hematoma or a break in the skin tissue of the canal wall. Additionally, thermal irritation of the periosteum of the bony canal may result from swimming in cold water, leading to the formation of bony growths or exostoses.
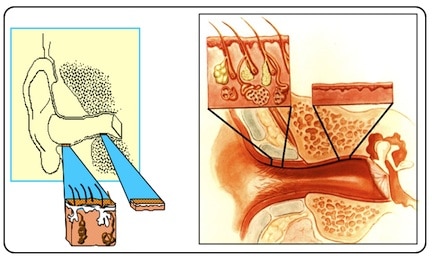
Figure 1. Skin thickness differences between the cartilaginous and bony canal portions, along with underlying substructure differences.
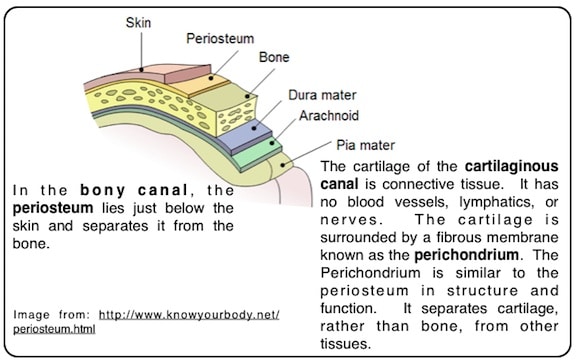
Figure 2. Illustration showing that in the ear canal, there is a layer of separation between the skin and the bordering bony and cartilage structures. In the osseous canal it is periosteum, and in the cartilaginous canal it is perichoncrium that forms this separation.
The cartilaginous portion of the ear canal has an underlying structure of cartilage, rather than bone. A fibrous membrane called the perichondrium that separates it from other tissues surrounds the cartilage. Cartilage is not as hard and rigid as bone, and hence, is more flexible and elastic. Cartilage is covered by a thicker skin lining (about 0.5 to 1 mm) than the osseous canal, and has a well-defined subcutaneous dermis layer (not present in the bony canal) as illustrated in Figures 3 and 4. Figure 3 is a generalized drawing of the human body skin composition.
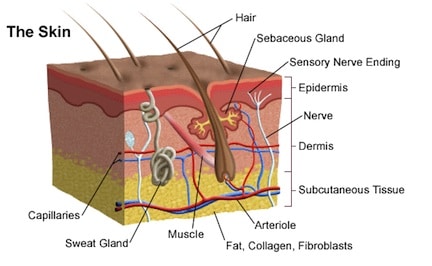
Figure 3. Generalized composition of human body skin (University of Miami Health Science System).
Figure 4 is an illustration of the epidermal and subcutaneous anatomy of the skin lining covering the cartilaginous ear canal. It shows a significantly deep layer of soft tissue that contributes to the expandability/displacement within the cartilaginous ear canal, and that allows many in-ear devices to be worn comfortably, even if they do not conform exactly to the ear canal architecture. Many hair follicles are found in the lateral one-third of the cartilaginous canal. The modified apocrine (ceruminous) and sebaceous glands develop from the outer root sheath of the air follicles exclusively in the skin lining the cartilaginous part of the ear canal.
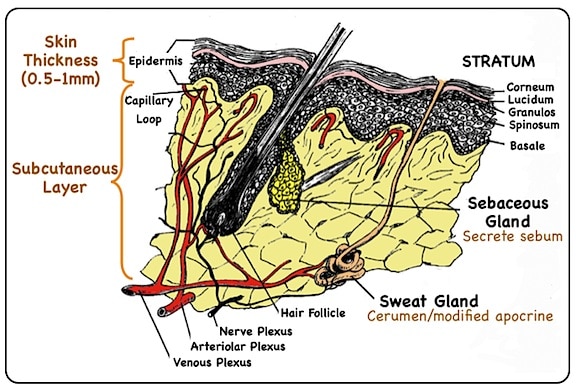
Figure 4. Detailed drawing of the skin layer of the cartilaginous ear canal. It is typical of general human body composition as seen in Figure 3. The cartilage lies beneath this subcutaneous layer.
The skin normally offers strong resistance to infection. It seems probable that the acidity of human sweat is responsible for killing most of the human pathogens by maintaining a skin pH of from 3.0 to 5.0. An increase in sweat reduces its acidity and disinfectant properties.
Canal Blood Supply
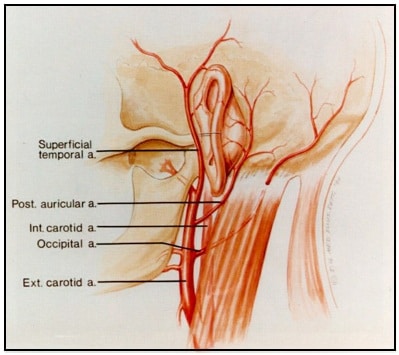
Figure 5. Illustration showing that the ear has an abundant blood supply made available through branches from the external carotid artery (Miyamoto and Miiyamoto, 1995) .
The ear has an abundant blood supply from the posterior auricular artery (extending from the external carotid artery) and from small auricular branches of the superficial temporal artery (Figures 5 and 6). From the superficial temporal artery, auricular branches are distributed to the lobule, anterior portion of the auricle, and to the external auditory meatus.
The meatus is partially supplied by the same vessels as the auricle, but the deeper portion, including the external surface of the tympanic membrane, is supplied by the deep auricular artery, a branch of the first (mandibular) portion of the internal maxillary artery. The veins accompany the arteries in course and name until they leave the region of the ear. The vein drainage is illustrated in Figure 7.
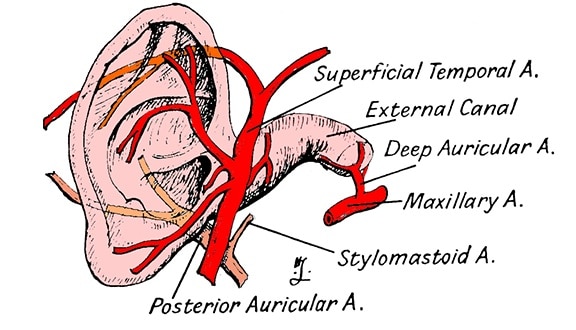
Figure 6. The blood supply to the ear, to be viewed with Figure 5 to gain an appreciation of its abundant blood supply, with the ear canal shown.
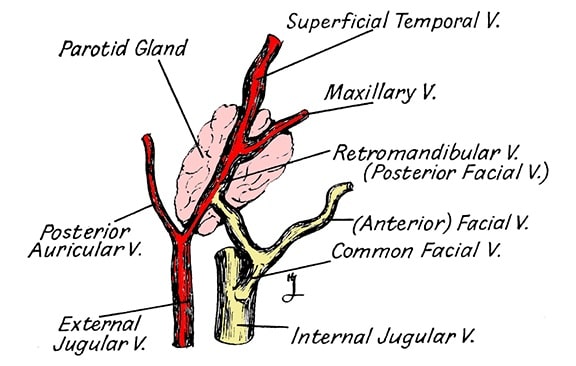
Figure 7. The venous drainage of the ear. It accompanies the arteries in course and name until it leaves the region of the ear.
Innervation
The sensory innervation of the auricle and ear canal is supplied primarily by branches of cranial nerves V and X, and from the cervical plexus, but it also receives branches from cranial nerves VII and IX (Figure 8). Because of overlapping of the auricle and ear canal innervated by these nerves and because of other natural variations, the precise distribution of these nerves is not constant
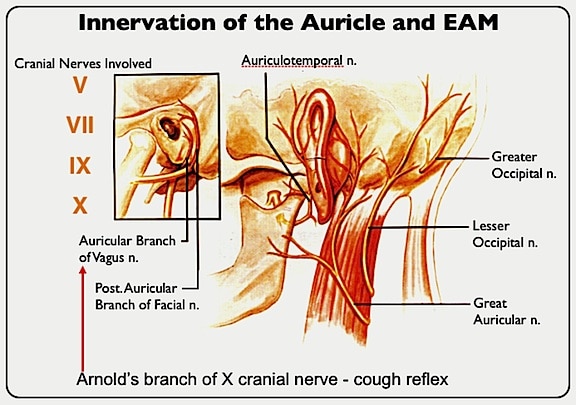
Figure 8. Innervation of the human ear. (Adapted from Miyamoto and Miyamoto, 1995).
Reference:
- Miyamoto, R., and Miyamoto, R. C. (1995). Pathology of the ear canal, Chapter 5 in The Human Ear Canal, Ballachanda, P (Ed.), Singular Pub. Co., San Diego, pp 53-82.
Wayne Staab, PhD, is an internationally recognized authority in hearing aids. As President of Dr. Wayne J. Staab and Associates, he is engaged in consulting, research, development, manufacturing, education, and marketing projects related to hearing. His professional career has included University teaching, hearing clinic work, hearing aid company management and sales, and extensive work with engineering in developing and bringing new technology and products to the discipline of hearing. This varied background allows him to couple manufacturing and business with the science of acoustics to bring innovative developments and insights to our discipline. Dr. Staab has authored numerous books, chapters, and articles related to hearing aids and their fitting, and is an internationally-requested presenter. He is a past President and past Executive Director of the American Auditory Society and a retired Fellow of the International Collegium of Rehabilitative Audiology.
**this piece has been updated for clarity. It originally published on July 21, 2014




