

Contraindications to Hearing Aid Use
Everyone recommending and fitting hearing aids is required by law (FDA, 1977) to determine if a patient has hearing conditions that could contraindicate hearing aid use, at least at the time when the fitting of hearing aids is being discussed. If any of the 8 red flags occur, referral to a physician is mandated, preferably to a physician specializing in diseases of the ear, where the issue may often be resolved with medical and/or surgical intervention.

While there are only eight conditions (called “The Eight Red Flags”), without reading from a form calling attention to each of these, dispensing hearing professionals relate that they often overlook some during their visual and interview stages. This is not intentional, but merely a result of not readily recalling each of them.
However, within each of these 8 red flags there exist numerous possibilities that must be considered. Therefore, it is good to have a systematic approach to navigate through the red flags.
Red Flags System: 3+2+3
Because of this, a number of years ago I developed a system for dispensing hearing professionals to use, and frankly, something I needed, when talking about the 8 Red Flags so that I could systematically move through the ear anatomy and conditions to identify each of the areas that needed to be reviewed. The system is simply called the 3+2+3.
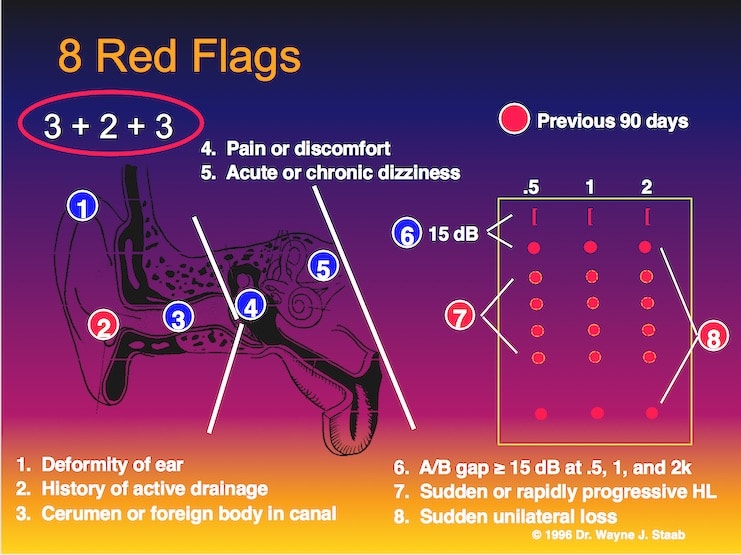
Figure 1. 2+3+2 Systematic Approach to navigate the 8 red flag medical contraindications mandated currently by the FDA.
Figure 1 uses a diagram of the ear as a backdrop to learn the system. The first number, ‘3’, relates to three issues related to the outer ear: (1) Deformity of the ear, (2) History of active drainage, and (3) Cerumen or foreign body in the canal.
Numbers 4 and 5 (the two ‘2′ middle numbers of the system) relate to issues in the middle ear and vestibular mechanism. Number 4 asks about any pain or discomfort associated with the hearing problem, and number 5 asks if he patient has acute or chronic dizziness.
The final number of the system, ‘3’, relates to three bits of information that can be taken from the audiogram and/or through inquiry. Number six calls attention to an air/bone gap. If equal to or greater than 15 dB at 500, 1000, and 2000 Hz, the patient is to be referred to a physician. Number seven alerts the clinician to watch for sudden or rapidly-progressive hearing loss, and number eight seeks to determine if the hearing loss is sudden, and unilateral.
The numbers in the red circles relate to any activity within the previous 90 days. Additionally, these red flag conditions can be determined through inquiry, actual observation, or review of any other available information.
Eight Red Flag Wording
The 3+2+3 study graph in Figure 1 uses some abbreviated wording. The actual wording for each of the red flags is as follows:
- Visible congenital or traumatic deformity of the ears
- History of active drainage from the ear within the previous 90 days
- Visible evidence of significant cerumen accumulation or a foreign body in the ear canal
- Pain or discomfort in the ear
- Acute or chronic dizziness
- Audiometric air-bone gap equal to or greater than 15 dB at 500, 1000, and 2000 Hz
- History of sudden or rapidly progressive hearing loss within the previous 90 days
- Unilateral hearing loss of sudden or recent onset within the previous 90 days
Not a Simple Process
Navigating the 8 Red Flags is not just some rapid, simple process, but one that requires a good understanding of normal and abnormal ear anatomy, physiology, and disease conditions. For example, under visible congenital or traumatic deformity of the ear, the hearing professional should be able to recognize whether the condition is due to acquired, traumatic, or congenital causes.
Entire lists of possibilities exist under this category alone (something for another post). This is the case with each of the other Red Flags, meaning that the dispensing practitioner be skilled in otoscopy, case history taking, and able to fully recognize potentially treatable conditions requiring medical referral.
Medical Evaluation Waiver
Fully informed adult patients may request the medical evaluation be waived for personal or religious beliefs. However, evaluation is mandatory for those under eighteen years of age. Additionally, if the person decides to forego the medical evaluation, he/she is still to be advised that exercise of the waiver is not in the user’s best health interest, and the dispensing party is prohibited from actively encouraging patients to exercise waiver option.
In practice, the waiver is used extensively by patients. This post will not address current controversy surrounding this issue. But, regardless of whether the necessity for a medical evaluation is modified by the FDA (Food and Drug Administration), it is still good practice to be able to systematically look for potential problems, and the 2+3+2 systematic approach presented in this post should always be applied – required or not.
(after publication of this article, in December 2016, the FDA Eliminated the Hearing Aid Medical Clearance Regulation)
Reference:
- Title 21- Food and Drugs, Chapter 1, FDA, Dept. HEW, Subchapter H, Medical Devices, Part 801 – Hearing Aid Devices; 801.420 – Professional and Patient Labeling; 801.421 – Conditions for Sale, Published: Federal Register, Vol. 42, No. 31, Tuesday, February 15, 1977, pp. 9286-9296




Pulsatile tinnitus is mostly associated with aneurysms, and not acoustic neuromas.
regards,
Jay Muhury