
Myth. “The ear impression otoblock stops the ear impression material from going too far into the ear canal, and protects the eardrum by not allowing it to come into contact with the eardrum.”
This post continues as background to show that the above statement is a myth, and a more realistic approach should be taken to the placement of the otoblock, and to explain the otoblock’s functional purpose.
Busted by Reality and Math
Ear Canal Length
Figure 1 shows the ear canal length from nine different studies using a variety of measurement procedures, but all on live individuals and/or ear impressions from the subjects1. The average canal length from these studies is 25.11 mm, with a range from 23 to 28.29 inches. It is known that female ear canals are about 3-4 mm shorter than male ear canals, but what is not known from the majority of studies, is whether the measurement length was from the aperture to the top, middle, or bottom of the tympanic membrane (eardrum). This alone can account easily for a 5-6 mm difference in length, with measurements made to the top of the eardrum being shorter, and those made to the full length (bottom) of the ear canal being longer. The assumption made in this post is that measurements were most logically made to either the center or bottom of the tympanic membrane.
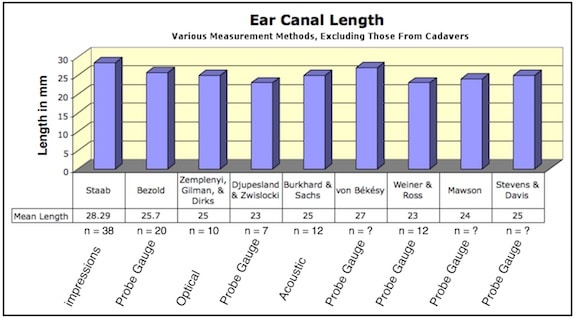
Figure 1. Ear canal length from nine studies that included male and female adult ears. The average is rounded to 25 mm.
Based on these results, this post will proceed with using an ear canal length of 25 mm as an “accepted” central TM average.
Now that we have some general dimensions for the ear canal, let’s turn to what the expectation should be when an otoblock/dam is placed in the ear canal so that it is “just past,” “a quarter of an inch,” or “2 to 5 mm” beyond the second bend, and not in contact with the tympanic membrane,” as is generally recommended.
Figure 2 shows the ear canal elongated essentially as a straight tube. Within the tube are lengths (in mm) from the aperture to the center of the first bend, ear canal isthmus, second bend, and eardrum length, assumed to be measured to the center of the tympanic membrane. The narrowing of the tube represents that expected at the isthmus. An otoblock compressed to just under 5 mm (from its original approximate 10 mm diameter) has been placed somewhere “beyond” the second bend of the ear canal.
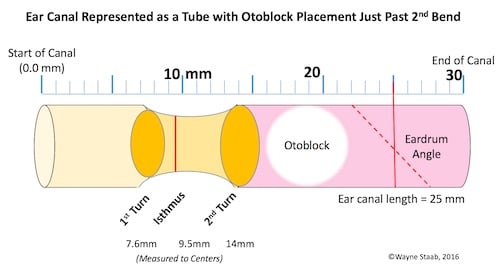
Figure 2. Average dimensional characteristics of an ear canal (elongated for illustrative purposes, except for the isthmus, where it narrows), first bend, isthmus, second bend, showing that the placement of an otoblock a “short” distance after the second bend, places the otoblock in close proximity to making contact with the tympanic membrane (TM), and in shorter ear canals, in direct contact with the TM.
Using average measurements for all of these features, it is obvious that the otoblock is easily within a couple of mm from coming in direct contact with the tympanic membrane, especially at the top and back (rear angle not shown, but it is closer to the otoblock than is the anterior edge of the tympanic membrane). Use of foam otoblocks (sometimes larger than cotton otoblocks), often result in jagged edges, some of which should almost make contact with the eardrum. With ear canals shorter (i.e., 20 to 22 mm in length), the otoblock may actually be in contact with the tympanic membrane, even if the person placing it does not think so.
What Does Placing the Block “Just Beyond” the Second Bend Mean?
Anatomically, the second bend is distal (closer to the tympanic membrane) than is the isthmus (Figure 2). The isthmus is the area at which the cartilaginous canal makes its transition to the bony canal. It also is often the narrowest portion of the ear canal, lying between the first and second turns of the ear canal, but slightly closer to the first turn.
How is “just past” the second bend determined, and even more specifically, “2-3 mm” past the second bend? Unless the person placing the block has some kind of magic “inside the ear canal” viewer that looks beyond the otoblock, this is just a poor guess, and often based on a false impression of the otoblock placed just beyond the isthmus, and not past the second bend. Many incorrectly think that when the otoblock “drops” behind a bend on insertion, that they are beyond the 2nd bend of the ear canal. This is a false assumption.
Why is This?
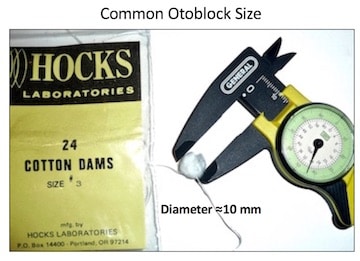
Figure 3. Cotton block (otoblock/dam) of average size (#3 Hocks) is approximately 10 mm in diameter.
A cotton block (or other type of block) of average size (#3 Hocks) is roughly 10 mm in diameter (Figure 3). If the average ear canal is about 25 mm in length, placing a block “just past” the second bend will place the block in contract with the tympanic membrane in essentially every case (Figure 4).
Unfortunately, many dispensers have a poor understanding of the ear canal anatomy. What they usually see, is the block passing through the isthmus (narrowing of the ear canal) between the first and second bends of the ear canal. This is where they stop the insertion process, not past the 2nd bend, as they believe.
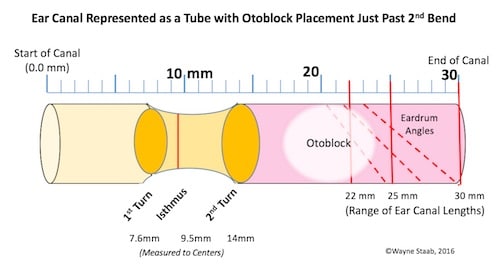
Figure 4. An otoblock placed 2 mm past the second bend of the ear canal will make contact with the TM for both a 22 and 25 mm long ear canal, and most likely even make contact in a 30 mm long ear canal. The range of 22 to 30 mm covers essentially the entire range of ear canal lengths.
A Good Ear Impression with Improper Otoblock Placement
Why do individuals sometimes still get a good ear impression even thought the block has been terminated in the wrong position, making them believe that they placed the block properly? This can be explained by viewing Figures 5 and 6.
Figure 5 illustrates the otoblock just past the isthmus. There is an unfortunate bad bit of advice associated with this placement. Some sources suggest pulling on the string attached to the otoblock to see if it is “secure,” (does not pull out easily), and if it does, to use a larger otoblock. The assumption is that the otoblock is past the second bend, and this would be confirmed with a gentle pull on the otoblock string. In some cases, the otoblock may seem secure in that resistance is felt. However, just because the otoblock finds resistance against gentle pulling when placed just past the isthmus, there is no guarantee that the otoblock is filling the area past the second bend.
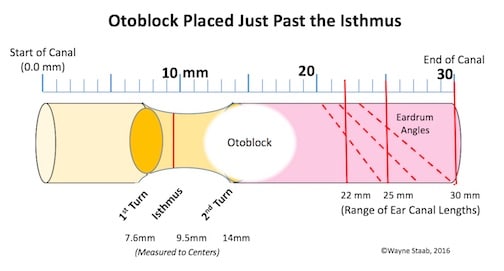
Figure 5. The otoblock most often is compressed when passing through the isthmus between the first and second bends of the ear canal during insertion. When this happens, the otoblock often seems to “disappear” and or “fall” into position as shown here. This provides a false sense of proper placement.
Figure 6 illustrates what happens with a poorly placed otoblock just past the isthmus. Upon insertion of the ear impression material, if the person’s head moves away from the injection, the ear impression material has pushed the otoblock against the TM, and this is represented as head movement. In some cases, the result can be a decent ear impression. But, this is not a preferred procedure – placement should not be based on hope and chance.
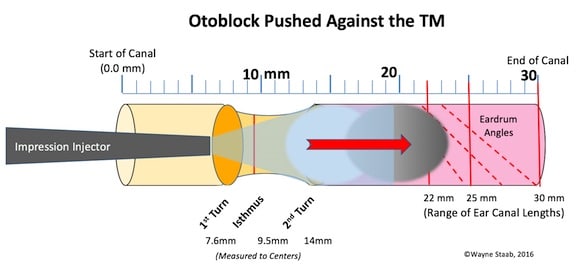
Figure 6. The effect of a poorly-placed otoblock just past the isthmus. Upon injection of ear impression material, the force of the injection can easily push the otoblock against the TM. Of course, this depends on the viscosity of the ear impression material, the type of injector, and the force used to inject the material. Regardless, if the subject’s head moves away from the injection process, you can be assured that the impression material has driven the otoblock against the TM.
A following post will conclude this series on the “Ear Impression Otoblock Myth” and provide logical justification for placing the otoblock against the eardrum initially, and intentionally.
Reference
- Staab, W.J. (2014). The human ear canal V, hearinghealthmatters.org, July 7.
Image, Plural Publishing Co.



