
This post provides an historical archive to the application of hearing aids. The auriculostomy may have been the first surgical hearing aid involvement in the fitting of amplification in that it provided an alternate approach to the application of corrective amplification involving ear-level hearing aids1. This was in 1975. It was an invention of Charles Strzalkowski, an innovative and creative hearing aid dispenser in Milwaukee, Wisconsin. Much of this was driven by Charlie’s desire to better overcome his severe bilateral sensorineural hearing impairment. However, Charlie needed someone to manufacture this instrument for him. That is where we, at Telex (where the author was at that time), entered into the picture where product design, electronics, drafting, tooling, molding, and assembly work was performed. An otolaryngologist in Milwaukee, J. Victor Bolger, performed the surgical procedure, called the auriculostomy.
The auriculostomy utilized a simple surgical procedure that allowed a hearing aid to be fitted in a specially-designed manner to allow for certain cosmetic, fixation, and instrument function improvements over conventional hearing aid fittings at the time. The hearing aid was patented originally in an eyeglass hearing aid arrangement2.
Description

Figure 1. The original commercially-available auriculostomy hearing instrument, in a BTE format. It had a mini plug extending directly from the hearing aid processor, through the fenestra, and into an earmold that extended the length of the concha where it coupled with the mini plug. (In this photo, the earmold is positioned incorrectly – upside down, and should be pointing upward, not downward).
The surgical office procedure for this fitting application was simple and performed under antiseptic conditions. A small fenestra (opening/window) in the posterior/inferior concha cavum of the auricle was made utilizing a special tool. The fenestra penetrated the two epithelial layers (anterior and posterior), two layers of perichondrium covering the auricular cartilage, and the cartilage itself. The surgical procedure to make this opening was called auriculostomy. Through this opening passed a connector that coupled the hearing aid (behind the ear) to a canal earmold that contained the hearing aid receiver/speaker (Figure 1). The canal earmold was originally constructed in such a way that its lateral projection rested at the fenestra opening, and connected with a direct plug-in. However, this was redesigned to remove most of the earmold for improved cosmetics as illustrated in Figure 2.

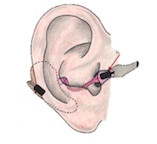
Figure 2. An iteration of the auriculostomy fitting in which the direct connection using a plug into a canal earmold that extended back to the fenestra was replaced with the electrical connection housed in a flexible plastic tube, run along the lower part of the concha, and then wired to a receiver positioned into a much smaller and less visible canal earmold in the opening of the external auditory meatus. The earmold no longer extended across the concha to the fenestra, leaving the concha essentially visibly open and unoccluded.
Advantages Driving This Technology
What were the reasons for performing such a radical approach to fitting hearing aids? The advantages were listed as follows:
- More severe hearing losses could be fitted with an ear-level, rather than body-worn hearing aid. What allowed this to happen was that this fitting allowed for more usable gain at the ear-level before acoustic feedback occurred. This was in part because the two transducers (microphone and receiver) were physically separated by distance, and also because the auricle was positioned between them. As a result, this fitting procedure could be used by individuals needing more usable gain than allowed from traditional ear-level fitting at the time, and who refused to wear body-worn instruments. This was meant also to circumvent power CROS fittings, a technique also intended to assist in controlling acoustic feedback (Figure 3).
- The hearing aid could be fixed to the auricle better for active persons. By coupling the hearing aid and in-ear parts through the auricle, the device was fixated to the ear of active persons, including children.
- The BTE hearing aid processor was not limited on fitting into the upper space between the auricle and the skull. Some individuals have little space between the auricle and skull, especially in the location where the hearing aid processor normally rests (Figure 4). The alternate anchoring approach used circumvented this issue. The Auriculostomy should work well for those who wear glasses, want a BTE hearing aid, but don’t like it when the hearing aid and the glasses temples compete with each other for the same real estate. However, eyeglass wearers were not as inclined to use such a fitting because it required that they remove the hearing aid every time they removed their eye glasses.
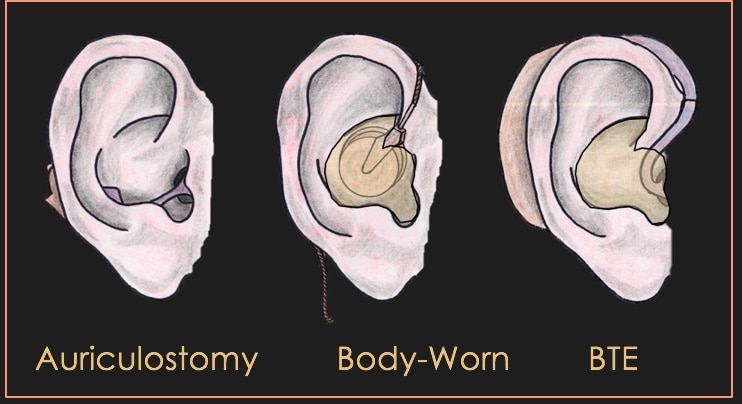
Figure 3. The auriculostomy fitting provided for a more cosmetic fitting because the mass of the earmold, the button receiver of a body-worn aid, and the hearing aid itself was better concealed.
- The auriculostomy would anchor the hearing aid to small ears. Keeping hearing aids on small ears of children has historically been a problem, especially the larger power BTE hearing aids used with those individuals having severe-to-profound hearing levels. A variety of head bands and other such securing techniques could be avoided.
- Improved cosmetic appeal. Some individuals prefer the more cosmetically-appeal of the auriculostomy because the connection to a canal earmold was not as obvious as that to a full shell earmold of traditional body-worn, behind-the-ear (BTE) or eyeglass hearing aids, and might even allow for a BTE fitting rather than a body-worn hearing aid because of its ability to manage feedback better.
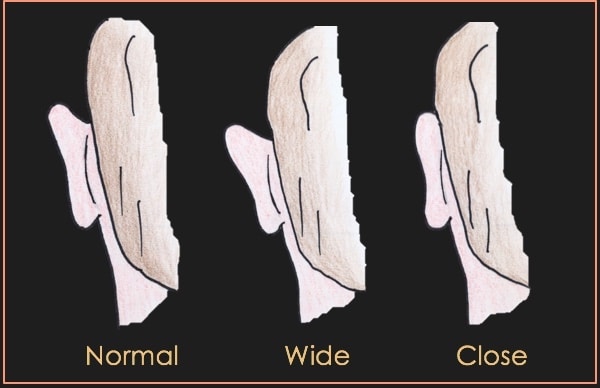
Figure 4. The auriculostomy fitting procedure moved the location of the hearing aid processor to a lower position behind the ear, thus keeping it from pushing out on the upper part of the auricle for individuals where the auricle fitted closely to the skull, and causing discomfort.
Auriculostomy continued next week, focusing on questions, and the actual procedure.
References
- Bolger JV, Strzalkowski CW, and Staab WJ. (1975). Auriculostomy. An alternate approach to the application of corrective amplification involving ear-level hearing aids. Hearing Instruments, February, 1975, pp 14-15.
- US Patent 3068954, 1962. Hearing aid apparatus and method.


