
In my last post, I made the statement, “Meniere’s is poorly understood and not very responsive to treatment intended to regulate fluid pressure within the labyrinth. There are several theories regarding the cause of Meniere’s symptoms, but no one knows for sure.” I say this based on literature review, my years of experience, and I reflect back on a ten part series I did on this blog in 2012 titled “Treatments for Meniere’s disease: Fact, Fiction, or Biological Plausibility.”
Things can change so quickly that I thought it wise to review that series, and update where necessary. I don’t think I will need ten parts for the update, but let’s begin.
I began the series discussing the use of betahistine, which is used frequently in the United Kingdom, but is not approved by the FDA in the United States. As of August, 2016, it is still not approved by the FDA and there is little additional research. There is one important additional study performed in Germany that was published in 2016. It seems to confirm the FDA opinion that Betahistine is safe, but probably ineffective in treating Meniere’s disease. Like many treatments for Meniere’s disease, they found no differences between the patients taking Betahistine and taking a placebo. Excerpts of the article and a link to the full article are pasted below.
There is one excerpt from the article that caught my eye, so I share it here:
“How betahistine might have an effect in the prophylactic treatment of Meniere’s disease is so far unknown. It could lead to an improvement of labyrinthine microcirculation, thereby rebalancing the production and resorption of endolymph. The drug was first registered in Europe in the 1970s and has been administered to more than 100 million patients so far.”
Think about that, no one is sure of the mechanism of action, there is no evidence that it makes a difference, yet over 100 million patients have been prescribed Betahistine. Here’s an excerpt from the abstract:
Efficacy and safety of betahistine treatment in patients with Meniere’s disease: primary results of a long term, multicentre, double blind, randomised, placebo controlled, dose defining trial (BEMED trial).
Adrion C1, Fischer CS2, Wagner J3, Gürkov R4, Mansmann U5, Strupp M6; BEMED Study Group
Participants received placebo (n=74), low dose betahistine (2 × 24 mg daily, (n=73)), or high dose betahistine (3 × 48 mg daily, (n=74)) over nine months. The primary outcome was the number of attacks per 30 days, based on patients’ diaries during a three month assessment period at months seven to nine. Secondary outcomes included the duration and severity of attacks, change in quality of life scores, and several observer-reported parameters to assess changes in audiological and vestibular function.
STUDY ANSWER AND LIMITATIONS:
Incidence of attacks related to Meniere’s disease did not differ between the three treatment groups.
I found a second study that is equally interesting. In 2014, JJ Nauta published a meta-analysis of 12 studies measuring efficacy of Betahistine for treating vertigo and Meniere’s disease. His conclusion was that Betahistine almost doubled the chances of reducing symptoms of vertigo compared to placebo. Journal reviewers (Database of Abstracts of Reviews of Effects (DARE) did not take kindly to what they apparently perceived to be biased and unsupported conclusions. The reviewers conclude:
“There were substantial limitations to the review, and there was little evidence, which was varied. Given these limitations, the treatment effect may have been overestimated. The author’s conclusions cannot, therefore, be considered to be reliable.
Conflict of Interests: The author was an employee of Abbott, a manufacturer of betahistine.”
It appears that betahistine, while widely used in Europe, is a harmless, but probably ineffective treatment for Meniere’s disease.
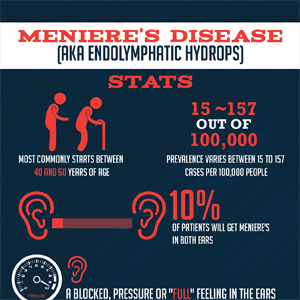
Photo courtesy of blog.earsinus.com



