
 Ear Canal Dimensions
Ear Canal Dimensions
Measurements of the human ear canal that show dimensional characteristics have been taken primarily from ear impressions. However, unless an impression is made of the entire ear canal, including the tympanic membrane, the length of the canal cannot be determined. A further weakness of ear impressions is that they do not show the dynamic changes in the ear canal resulting from mastication, speaking, etc.
Regardless, some of the measurements provide rather good generalized information about the ear canal.
Ear Canal Length – Cadaver vs. Live Measurements
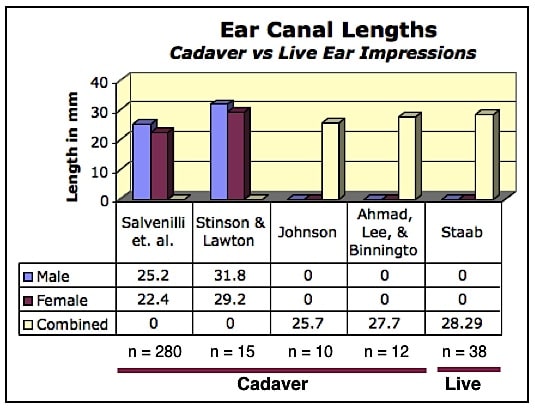
Figure 1. Average human ear canal lengths reported by various researchers. The reported length measurements depend upon two factors: (1) the specific location of the aperture, and (2) the point on the tympanic membrane to where the measurement is made. Comparing length measurement from cadaver ear impressions to those made on live individuals, it would appear that concerns related to comparing measurements might be ignored.
Measurements of ear canal length from ear impressions require that the entire canal be included, including the tympanic membrane. As such, measurements have been obtained from ear impressions made of: (1) cadaver ears, and (2) ear impressions of live individuals – the latter requiring special skills and materials. However, are measurements of ear impressions of these two different categories really comparable? Do cadaver ears shrink and/or create other potential changes that may not be representative of live ears?
Figure 1 shows average ear canal lengths measured from four cadaver ear impression studies compared to one study that made measurements from ear impressions made on live individuals. Because the exact proximal and distal measurement locations were not always specified, the data cannot be directly compared. However, the range from the four cadaver studies shows the average to be between 22.4 and 31.8 mm. Data from Salvenilli, et. al., and Stinson and Lawton provide averages for both males and female subjects, whereas Johnson and Ahmad, et. al. provide combined gender data. The study on live individuals (Staab, 1993) showed averages that fell within the range of that for cadaver ears, suggesting that cadaver and live ear data could be combined. The live ear data measurements were made from the aperture of the ear canal to the most distal point of the ear impression. Of interest is that it appears that the length difference between male and female ear canals is approximately 2 mm, with male ear canals longer. This is consistent with other data and will be reviewed later in this post.
Ear Canal Length – Measurement Method Comparisons
A previous post described different methods for making ear canal measurements, especially those related to length. Results of various measurements are shown in Figure 2, without the cadaver ear measurements from Figure 1. This includes measurement averages reported, and excludes those that reported the length in ranges but with averages not given. The length ranges from 23 to 28.29 mm. When using a probe to make ear canal measurements, it seems logical that the probe is most likely to contact the center of the TM (umbo), or adjacent portions of the TM, and report shorter lengths than those that measure to the most distal point of the ear canal, such as those by Staab. Of course, regardless of what the distal measurement point is, the proximal measurement location (aperture opening) can have a significant impact as well. There is no exact anatomical designation of the aperture. As such, that designation is subjectively determined by the measurer.
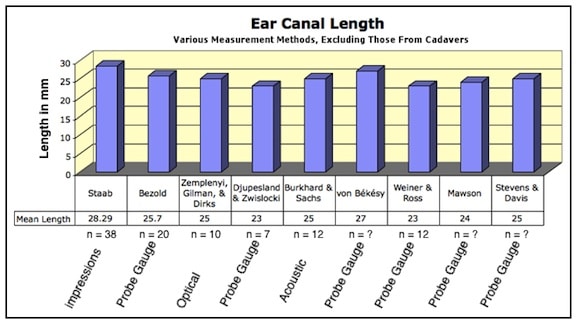
Figure 2. Ear canal length averages excluding those made on cadaver ear impressions shown in Figure 1. Some measurements suspected to have been made to the umbo, or middle of the tympanic membrane, are shorter.
Ear Canal Length – Gender Differences
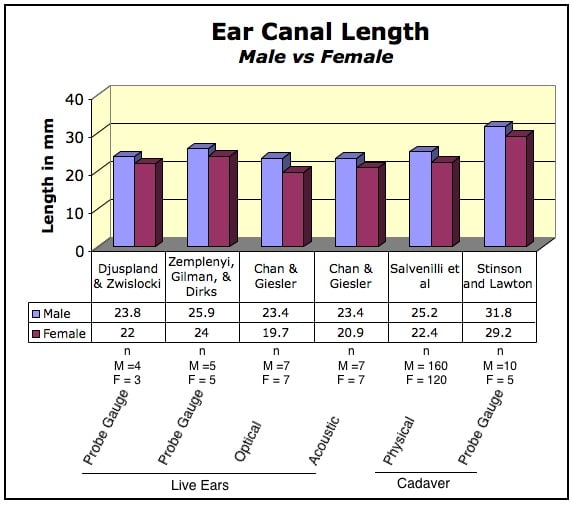
Figure 3. Gender differences in human ear canal length, with male ear canals showing greater length, regardless of the measurement method.
A gender difference in ear canal length was suggested in Figure 1, with male ear canals longer than female ear canals. This is explored further with results provided in Figure 3. In all cases, whether cadaver or live ear measurements, male ear canals were longer by a range of 1.8 to 3.7 mm. This trend was consistent, regardless of the measurement method.
Ear Canal Configuration Measurements
Ear canal length is an interesting measurement, but generally has little to do with how various earpieces fit into the ear canal. Of greater importance are the internal dimensions that determine how much real estate is available, and what areas are most subject to discomfort, cosmetics, security, and ill fit. Three measurements of significance are: (1) the aperture, or opening of the ear canal, (2) the isthmus, and (3) the area beyond the isthmus, leading to the tympanic membrane.
Ear Canal Aperture Measurements
The aperture is the opening exiting the concha into the ear canal. The aperture size (width and height) are often limiting dimensions to hearing aids, earbuds, and other devices that deliver sound (or prevent sound, as in the case of earplugs) into the ear canal. Figure 4 is a histogram of human ear canal aperture openings (height in blue, and width in orange), reported by various studies. Thomas, W., Wright, W., & Casali, J. Earcanal measurement: Eargage™ versus ear impressions. Spectrum, 11(1), 34-35 (1994). These measurements are taken essentially from ear impressions. The key is as follows:
• Europe = White, European descendants, from US, Canada, and Europe
• M = Male
• F = Female
• Mixed = Male and Female combined
• Chinese = Measurements obtained from Chinese (Hong Kong) individuals
• Japanese = Measurements obtained from Japanese (Tokyo) individuals
• African = Black individuals, regardless of country
• Asian = Specific country not identified
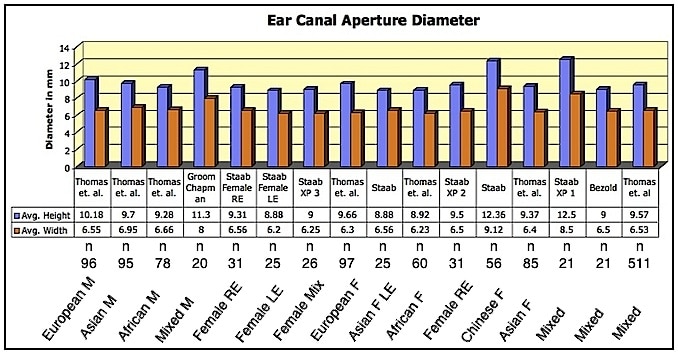
Figure 4. Ear canal aperture diameter averages for height (blue) and width (orange) as reported by various authors. In addition to the number in the populations investigated (n), ethnic groups are identified.
In all reports used in Figure 4, the ear canal aperture height is greater than the width. The height ranges from 8.88 to 12.5 mm, while the width ranges from 5.7 to 9.12 mm. It is not appropriate to average the averages, but the height appears to be around 8.5 mm, and the width around 6 mm. Regardless of the gender or ethnicity, dimensional trends are fairly similar. However, Thomas et al. reported that in their study ear canals in people of European descent are significantly larger than in those of Asian descent, which are significantly larger than in those of African descent. The general shape is oval. The data from Staab features mostly female ears. That is because the goal was to determine the smallest ear canal sizes (other than children’s) that existing electronic components could be placed into a listening device when fitted deeply into the ear canal.
The two greatest dimensional measurements by Staab (height averages of 12.36 and 12.5 mm) reflect an intentional attempt to enlarge the aperture by “stretching” the opening using a denser and harder silicone paste (70 Shore A) ear impression material. This was done to provide additional space in the expandable cartilaginous region of the canal for electronic component placement. Expansion of the cartilaginous ear canal by making the ear impression with a high Shore (70) versus a low Shore (20) by Termeer showed as much as 100% width expansion when using the higher Shore impression material (Figure 5).
Two impressions were made of each ear – a 70 and 20 Shore impression. (Shore refers to the end hardness of the impression). The 20 Shore impression material was injected with essentially no pressure, while the 70 Shore A impression material was produced under 150 grams of pressure at the outlet of a standard silicone syringe. However, about 50% of the 108 subjects showed expansion of 20% or less when the impression was made with the 70 Shore impression material. Assuming an approximate 6.5 mm aperture width, this would result in an expansion of 1.3 mm (to 7.8 mm). The interest was in the width rather than the height because it was the smallest dimension and most likely to require additional expansion for component introduction.
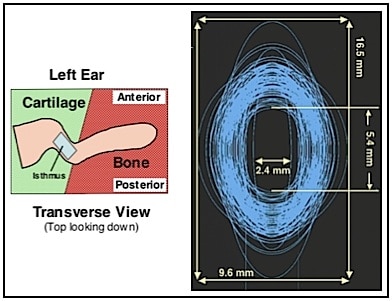
Figure 6. Elliptical plotting of the isthmus of each of the adult ear impression measurements from Staab and Sjursen (2000) to provide a visualization of the range of data from their study (n = 112). The left image shows the approximate location of the isthmus for reference, as viewed from the top looking down.
Ear Canal Isthmus Measurements
The isthmus of the ear canal is generally the narrowest portion of the ear canal, and is in close proximity to the second bend. This area is also impacted by movement of the mandible. As a result, designing a device to fit through the isthmus area requires a firm understanding of how the isthmus impacts devices designed to pass through that area. The average height is close to 9 mm, and the average width about 5.7 mm (Figure 6). Figure 6 shows an elliptical plotting of each of the measurements from Staab and Sjursen to provide a visualization of the range of data from their study.
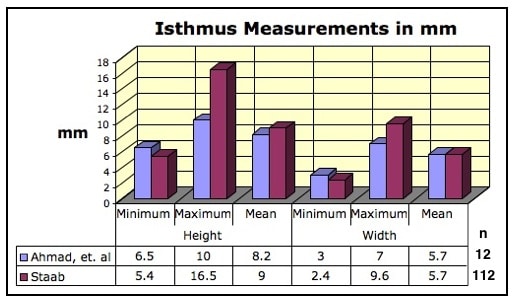
Figure 6. Human ear canal isthmus measurements of height and width (minimum, maximum, and mean results).
The Ear Canal – Beyond the Isthmus
Little information is available relative to the dimensions of the ear canal beyond the isthmus. Still, this is important information, especially as instruments fit more deeply into the ear canal, and especially when they terminate medial to the isthmus. One potential advantage of placement beyond the isthmus is that the ear dynamics are less in play because of the hard, bony lining of that portion of the canal – meaning that mandibular movement is not expected to come into play, especially if the inserted device is beyond the isthmus. Therefore, any measurement for a given individual should be static. However, that can also lead to greater discomfort (discussed in a following blog of this same series). Figure 7 provides the minimum, mean, and maximum diameters of the ear canal just before the tympanic membrane (Near TM measurements) as recorded from 21 ear impressions of the complete ear canal, including the TM). For this population, the height and width are essentially the same as at the isthmus. The height minimum, mean, and maximum were 6.25, 8.2, and 10.1 mm. The width minimum, mean and maximum dimensions were 4.5, 6, and 7 mm.
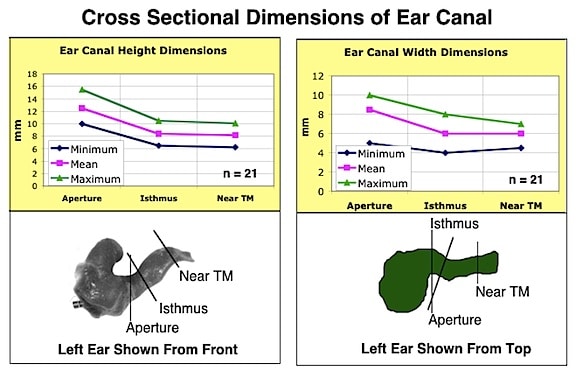
Figure 7. The primary area of interest in this graphic relates to the dimensions immediately prior to the tympanic membrane (Near TM). The average height is 8.2 mm and the average width is 6 mm (Staab,, 2002).
Reference:
- Salvinelli, Maurizi, Calamita, D’Alatri, Capelli, and Carbone. (1991). Scandinavian Audiology, Vol. 20:253-256
- Stinson, M., and Lawton, B. (1988). Specification of the Geometry of the Human Ear Canal for the Prediction of Sound-Pressure Level Distribution, Journal of the Acoustical Society of America, vol. 85, No. 6, June 1989, pp 2492-2503
- Djupesland, G. and Zwislocki, J.J. Sound pressure distribution in the outer ear. Scan. Audiol. , 1(4):197{203, 1972
- Zemplenyi, J., Gilman, S., and Dirks, D. Optical method for measurement of ear canal length. J. Acoust. Soc. Am. , 78(4):2146{2148, 1985
- Chan, J.C,, & Geisler, C.D. Estimation of eardrum acoustic pressure and of ear canal length from remote points in the canal. J Acoust Soc Am. 1990 Mar;87(3):1237-47
- Salvinelli, Maurizi, Calamita, D’Alatri, Capelli, and Carbone. (1991). Scandinavian Audiology, Vol. 20:253-256
- Stinson, M., and Lawton, B. (1988). Specification of the Geometry of the Human Ear Canal for the Prediction of Sound-Pressure Level Distribution, Journal of the Acoustical Society of America, vol. 85, No. 6, June 1989, pp 2492-2503
- Termeer, P. (1994). Philips Hearing Instruments Internal Research Document
- Staab, W.J. and Sjursen, W. (2000). A one-size disposable hearing aid, American Auditory Society, March, Scottsdale, AZ
- Groom, D, and Chapman, W. (1959). Circulation, Journal of the American Heart Association, 19:606-608
- Bezold, R. (1882). Die Corrosions-Anatomie des Ohres
- Staab, W. Asian ear canal dimensions and the relationship to a stock ITC hearing aid. Special Physician Group, Nagasaki, Japan, June 2002
- Staab,W. Ear Impression Results on 100+ Peritympanic Patients, Colorado Otology/Audiology Conference, Breckenridge, Colorado, March 1993
- Bezold, R. (1882). Die Corrosions-Anatomie des Ohres
- Zemplenyi, J., Gilman, S., and Dirks, D. Optical method for measurement of ear canal length. J. Acoust. Soc. Am. , 78(4):2146{2148, 1985
- Djupesland, G. and Zwislocki, J.J. Sound pressure distribution in the outer ear. Scan. Audiol. , 1(4):197{203, 1972
- von Békésy, G. (1960). Experiments in Hearing. McGraw-Hill Book Co. NY
- Weiner, F.M., and Ross, D.A. (1946). The pressure distribution in the auditory canal in a progressive sound field. JASA Vol. 18, No. 2 (Oct.), pp. 401- 408
- Mawson, Stuart R., 2nd ed. London: Edward Arnold, 1967
- Stevens, S., and Davis, H. (1938). Hearing: Its Psychology and Physiology, John Wiley & Sons, Inc., New York
- Johansen, P. (1975). Measurement of the human ear canal. Acustica, 33, pp 349-351
- Ahmad, Ijaz, Lee, W.C., Binnington, J.D. (2000). External Auditory Canal Measurements: Localization of the Isthmus, Otorhinolaryngology Nova 2000: 10:183-186 (DOI: 10.1159/000054815)
- Staab, W. Ear Impression Results on 100+ Peritympanic Patients, Colorado Otology/Audiology Conference, Breckenridge, Colorado, March, 1993
Wayne Staab, PhD, is an internationally recognized authority in hearing aids. As President of Dr. Wayne J. Staab and Associates, he is engaged in consulting, research, development, manufacturing, education, and marketing projects related to hearing. His professional career has included University teaching, hearing clinic work, hearing aid company management and sales, and extensive work with engineering in developing and bringing new technology and products to the discipline of hearing. This varied background allows him to couple manufacturing and business with the science of acoustics to bring innovative developments and insights to our discipline. Dr. Staab has authored numerous books, chapters, and articles related to hearing aids and their fitting, and is an internationally-requested presenter. He is a past President and past Executive Director of the American Auditory Society and a retired Fellow of the International Collegium of Rehabilitative Audiology.
**this piece has been updated for clarity. It originally published on July 7, 2014



