
Anterior canal BPPV is quite rare, and is estimated to account for 1 to 2% of cases of BPPV. The primary diagnostic feature is the fact that the nystagmus associated with anterior canal BPPV is torsional and downbeating, whereas the more common posterior canal BPPV nystagmus is torsional and upbeating. This is not always easy to detect with the naked eye, so there is an advantage to using video-oculography to amplify, replay and analyze the nystagmus response to the Dix-Hallpike provoking manuever.
The anatomy of the labyrinth is such that loose otoconia particles naturally gravitate into the posterior canal when the patient is supine. In order for the particles to enter the anterior canal (also known as the superior canal), the head has to be almost upside down.
Since getting the head close to upside down is a goal of canalith repositioning for the more common posterior canal BPPV, it is my belief that anterior canal BPPV is most often a complication of the canalith reposition procedure (CRP). I believe this to be the case in the patient described in the previous few posts.
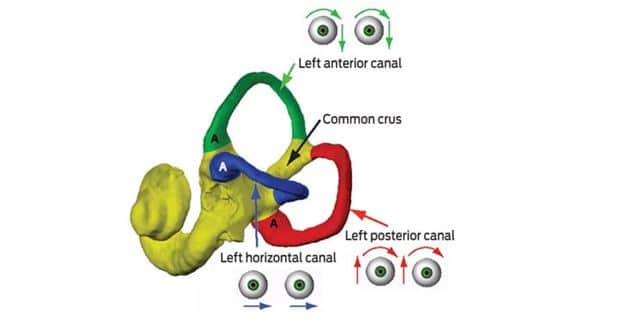
The anterior canal in one ear lies in the same plane as the posterior canal of the opposite ear. These planes are often described based on the involved pair of canals. For example, when the head is turned to the left and the eyes are directed forward, a vertical nod of the head will stimulate the right anterior canal and the left posterior canal simultaneously. This is known as the RALP plane (Right Anterior, Left Posterior). Conversely, the same vertical nod with the head turned to the right will stimulate the LARP plane (Left Anterior, Right Posterior).
The point here is that when you do a right Dix-Hallpike exam with the intention of stimulating the right posterior canal, you are also simultaneously stimulating the left anterior canal. Particles in either canal can trigger vertigo and a nystagmus response.
*Photo courtesy of the Medical Journal of Australia.


