
Hearing Healthcare Market Development Column
Covid-19’s mandate for social distancing greatly increases consumer-patient demand for an end-to-end hearing aid solution at home, from prescribing through care. In response to this structural change, Auditory Insight has analyzed close to 20 online hearing tests offered by global hearing aid brands and D2C hearing aid companies.
Our analysis showed that Shoebox Online, an online hearing screener, demonstrated two important best practices:
- A rigorous methodology to improve test accuracy by characterizing user hardware
- A clean, understandable user interface.
Auditory Insight defines an online hearing test as an assessment which consumer-patients take using their own PC or smartphone. Some online tests require headphones, others permit use of device speakers. Occasionally these tests display results in a typical audiogram, although more often they rely on broader categories.
Auditory Insight’s test taker was a male with a moderate, downward sloping hearing loss. Screenshots of every interaction went into a database in order to analyze the tests along a holistic set of dimensions. The purpose of the analysis was not to clinically validate the tests’ accuracy but rather to understand their design, user interface, and role within the company’s larger hearing aid marketing strategy.
Shoebox Online offers hearing care professionals (HCPs) the ability to perform a hearing screener remotely as part of a tele-audiology solution, permitted by some states during the coronavirus pandemic. However, Shoebox Online does not comply with some state regulations for diagnostic hearing testing which can require otoscopy, as well as bone conduction, and word recognition testing. HCPs should contact their state licensure boards to ensure compliance before engaging in online hearing testing activities.
Shoebox Online Hearing Test
Shoebox launched its online hearing test on April 15 of this year, during the heart of what may prove to be the first wave of the Covid-19 pandemic. A month later, on May 14, Signia announced its new Remote Care program which enables HCPs to “prescribe, fit, and fine-tune hearing aids remotely”. Signia’s Remote Care resource center recommends that for new patients or for those whose audiogram on file is more than six months old, an “online assessment via [the] Shoebox test.”
Although Shoebox is wholly owned by WS Audiology, it operates independently of the hearing aid business. Shoebox has several other solutions, including a tablet audiometer which allows full diagnostic pure tone and speech testing outside of a sound booth.
A major concern for HCPs is the accuracy of online hearing tests as compared to those administered with a calibrated audiometer. “The primary challenge with online hearing tests,” acknowledged Mike Weider, Shoebox’s chief executive officer, in a Zoom video interview, “is that we don’t have a known set of hardware.” Shoebox technology auto-detects whether the user is on a PC or mobile device, but the headphones type—in ear vs. on ear, wired vs. wireless—not to mention the headphones brand, are opaque.
To tackle this difficulty, Shoebox tested dozens and dozens of combinations of PCs and headphones to measure the sound output of each pairing. The goal was to delineate the universe of equipment. “It’s a harder problem than you might initially assume,” Weider said.
During the test itself, Shoebox collects information from the consumer-patient about their headphone type, as well as four other categories of input. Of this information gathered from the user during the test, perhaps most interesting is a dynamic range test.
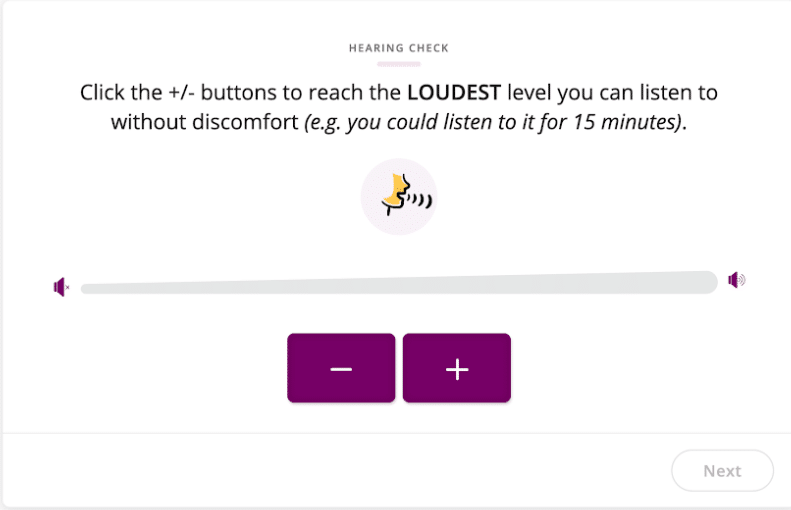
The Shoebox test asks the user to adjust a slider, until they reach “the loudest level you can listen to without discomfort (e.g. you could listen to it for 15 minutes).”
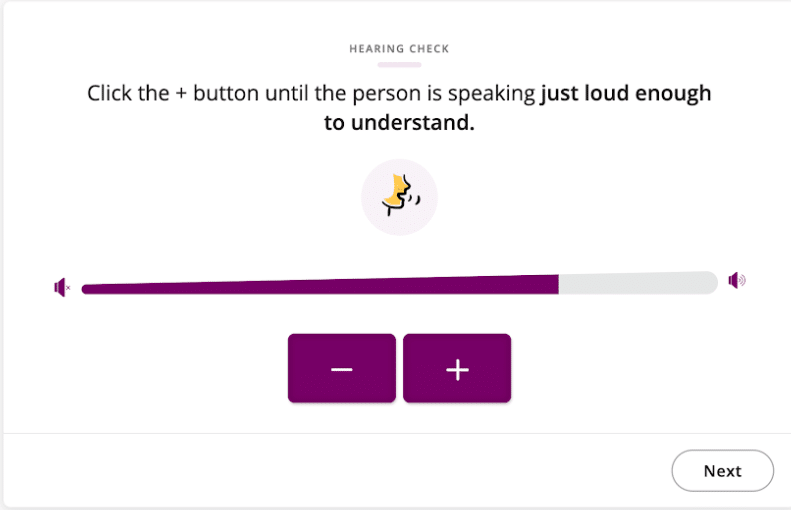
On the following screen, users must manipulate the slider until “the person is speaking just loud enough to understand.”
Weider explained that the underlying principle for the dynamic range test was pioneered by Dr. Frances Kuk, Ph.D., currently Vice President, Audiology, at Widex. The greater an individual’s hearing loss, the smaller the dynamic range for that individual between sounds that appear loud versus sounds that appear soft. Since the test measures the relative difference between two values, Weider said, “it is immune to hardware variability.”
Based on these four categories of input, the Shoebox test places users into three buckets: “Significant Loss,” roughly corresponding to a severe or profound hearing loss, “Loss,” roughly corresponding to a mild or moderate hearing loss, and “No Loss.” “The test computes a probability of where the user falls,” said Weider. “We’ve validated this model by comparing results to clinical audiograms,” he noted in a follow-up email.
The Shoebox test combines this technical depth with an elegant and effective user interface. The test provides users with clear instructions, a minimum of text, and appealing graphics.
“We want to make this available on a worldwide basis and in many languages,” Weider concluded. “There’s a lot of room for innovation still.”
**Disclosure: The author discloses that her company consults with hearing device manufacturers and pharmaceutical hearing healthcare companies
 Nancy M. Williams is President of Auditory Insight, a boutique consultancy advising leaders on transforming hearing healthcare. Nancy partners with senior leaders of pharma and device companies to develop successful commercialization strategies based on deep insight into patient needs, practical understanding of clinical behaviors of audiologists and ENTs, and unique viewpoints on how hearing healthcare is evolving. She holds an MBA from Harvard Business School and a B.A. from Stanford University in Quantitative Economics, both with distinction.
Nancy M. Williams is President of Auditory Insight, a boutique consultancy advising leaders on transforming hearing healthcare. Nancy partners with senior leaders of pharma and device companies to develop successful commercialization strategies based on deep insight into patient needs, practical understanding of clinical behaviors of audiologists and ENTs, and unique viewpoints on how hearing healthcare is evolving. She holds an MBA from Harvard Business School and a B.A. from Stanford University in Quantitative Economics, both with distinction.
*featured image courtesy Shoebox



With the use of computer chip technology in todays hearing aids, hearing tests will soon become a thing of the past. Testing , whether at the office or online will not only be unnecessary, but rendered obsolete as we explore hearing aid adjustments through speech understanding response patterns. We already know the various pathologies that are present and straightforward solutions to address them with current generation hearing aids. All that remains is to analyse cognitive actions and its variations that affect brain performance outcomes. Speech degradation mostly begins when the hearing thresholds reach or cross below 60db in most hearing losses. There are cases when neural configurations are affected by the use of reckless and careless hearing aid and connectivity uses. Such cases patients do need verbal counseling on select strategies. This will necessarily involve multiple visits, and use of remote connectivity is not the solution to helping with cognitive gains through HA amplification. So telemedicine does not help solve problems without frequent counseling !