
From HHTM Staff: Hansen’s disease, aka leprosy, is the subject of a multi-post chapter in HHTM Staff contribution series on transmittable but mysterious diseases that affect the body in different, often chronic ways, including the hearing and balance systems.
Today’s post continues the primer on Hansen’s, compiling basic information that Audiologists and other health professionals need to know when managing care of a patient with the disease or a history that suggests leprosy as a diagnosis.
Recap so Far
Hansen’s disease is caused by a bacteria that cannot be cultured in vitro, but thrives as a parasite in the human body. Once ensconced, it hides from the immune system–sometimes for years–by staying beneath the immunity system’s radar, then emerging as a variety of chronic, non-life threatening ailments that mimic other diseases and conditions. As a result, Hansen’s is hard to diagnosis, hard to study, and remains poorly understood.
Leprosy is more common in underdeveloped countries, but it is globally endemic. More than a hundred cases are identified in the US each year but the diagnosis is often delayed due to practitioners’ lack of knowledge about the disease. Thus, it is a “neglected” but potentially eradicable disease that is likely to increase in prevalence in developed countries as global vacations and business travel increase. The disease is more common in developing countries, with thousands of cases identified each year, perhaps at earlier stages, due to medical familiarity with the disease.
Leprosy’s transmission mode is unknown, but is now thought to rely on person-to-person spread via nasal droplets. Other possibilities are by skin or insect bites. Those receiving treatment for the disease are not infectious. Most people have a natural resistance and either don’t get it or are cured spontaneously. About 5% of people lack resistance due to defective cellular DNA. Those who lack resistance can contract the disease at any time in life; men are about twice as likely as women to get it, though the odds are equal or lean slightly to females in some parts of Africa.
What Does It Do?
The better question is “What does it NOT do?” It does NOT cause fingers, toes, or noses fall off, despite age-old beliefs in that regard.
There are a number of different kinds/classification of leprosy
, all beyond the scope of these posts and the practice of Audiologists. But, symptoms are common to the different types. In general, it can be said that leprosy damages peripheral nerves and that early diagnosis and treatment can prevent nerve damage and associated disabilities.
Hansen’s disease is “remarkably” hard to identify because symptoms can be subtle and diverse. The state of the person’s immune system and its response to infection determines how the disease manifests. Chronic and co-morbid infections are common; some symptoms mimic tuberculosis (Chow & Roman, 2008). Affected areas are peripheral, primarily on the skin, the mucous membranes, eyes, ears, testes, and peripheral nervous system.
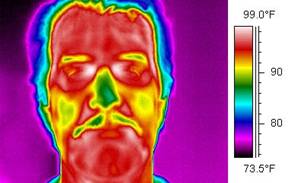
Figure 2. Cooler areas of the body (blue to violet) are where lepra nodules are most prevalent.
Numbness is the first symptom in a reported 90% of cases (Ngan). Scaly nodules eventually become visible, but sometimes not until years after the numbness first presents. The nodules are called “lepra” after the Greek work for scales. Chronic infections of the skin, eyes, and mucous membranes can occur.
Sensation is lost as destruction of peripheral sensory nerves progresses. The losses begin at the extremities. Temperature sensation goes first, followed by light touch, then pain and deep pressure awareness are lost. Peripheral neuropathy puts extremities at risk for trauma, injury, infection, and amputation (accidental or purposeful). This explains the false perception that leprosy cause dropped digits.
Ears are at high risk, too. Lepra lesions are more prevalent in skin regions that are below central body temperature, such as cartilaginous parts of the body. For this reason, the nose and ears are prime locations for leprosy lesions.
The infrared image of Figure 2 shows cooler areas of the body that correspond to common targets of leprosy and the feature photo in the title of this post shows leprosy lesions on ear cartilage — characterized as “smooth, shiny, diffuse thickening of the ear.”
Next Questions
The next question is “How does the leprosy bacteria destroy without killing its human host?” And, audiologically, is ear destruction limited to the outer ear cartilage or are the peripheral portions of the hearing/balance nerve at risk as well? Tune in next post for more on these topics.
References
Chow E & Roman T. Hansen’s disease in Londrina City: a public health intervention of leprosy in Brazil. Parasites and pestilence. Unpublished paper, Spring 2008.
Ngan, V. Leprosy (Hansen disease). DermNet NZ (June 9 2014).
Spierings E, et al. The role of Schwann cells, T cells and Mycobacterium leprae in the immunopathogenesis of nerve damage in leprosy. Lepr Rev. 2000 Dec;71 Suppl:S121-9.
feature Image courtesy of Wikipedia




