

Ear Impression Block Placement – The Otoblock Myth Busted by Reality
Opening Salvo
Most documents that instruct individuals on how to take ear impressions provide some misleading information, especially when describing the purpose and placement of the otoblock/block/dam/otostop. This series of posts is intended to show how the otoblok myth is busted by reality. Let’s look at some of the statements related to the ear impression block placement, and eventually explain how these statements help create the myth.
“Do not place the block on the eardrum. The block should be a quarter-inch beyond the second bend, just into the bony portion of the canal.”1
“The block should be at or past the second bend, in order to provide an accurate representation of the canal.”2
“Using a clean self-illuminated pushrod or ear light the otostop should be inserted into the ear canal normally to a point just beyond the second bend, i.e. approximately one-half of the way along the canal, although a shorter impression might be acceptable in some circumstances and it is important not to insert the otostop deeper than required as this can cause unnecessary discomfort and possible injury.”3
“A foam block is inserted to protect the eardrum.”4
“…an otoblock is gently placed beyond the second bend of the ear canal.”5
They Live Among Us
And then, you may find something like the following, which suggests that they are born and live among us:
“The ‘otoblock’ is a small, shaped piece of foam with string attached at one end. It is used to temporarily block the opening to the inner ear so that no impression material can enter the ear canal. …..and positioned in each ear just beyond the second bend in the ear…”6
It is rather difficult to imagine taking an ear impression without injecting ear impression material into the ear canal, and one would hope that the block is not inserted so deeply that it is used to temporarily block the inner ear.
Essentially, documents related to taking ear impressions almost always state something like the following: Place the block just past the second bend of the ear canal, but be careful not to have it come in contact with the eardrum.
This series of posts (this being the first) is intended to provide the background and information relative to ear impression otoblock placement, and to bust the myth regarding the statements posted above. To do this the reader will be walked through a number of steps/concepts leading up to destroying the myth, and resulting in a logical solution – one that takes the guesswork out of what most dispensers have been taught.
So, let’s start with some basics.
Landmarks and Dimensions of Interest
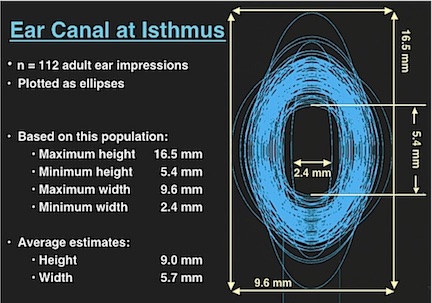
Figure 1. Dimensions of the isthmus, taken from 112 adult ear impressions, and plotted as ellipses. The average height was 9.0 mm, and the average height was 5.7 mm.
Isthmus – This is the transitional area of the ear canal from a cartilage lining to a bony lining, and lies between the first and second bends. It is often the narrowest part of the ear canal, but can vary widely (Figure 1)7.
In addition to the diameter of the isthmus, its location is of interest as well. Interestingly, little measured/reported data is available, a curiosity in itself, considering all the attention to the ear canal when making ear impressions.
To gain a perspective of how the ear canal isthmus and other parts of the ear canal are involved in the placement of the otoblock, Figure 2 shows the results of actual measurements of the isthmus location in mm from the aperture (opening) of the ear canal. The isthmus lies about 9.5 mm from the aperture of the ear canal (but has been reported to be as close as 7 mm). Because the isthmus is where the bony ear canal starts its transition to take over as the “housing” of the ear canal, this shows that the cartilaginous portion is approximately 1/3 of the ear canal, and that the bony section comprises about 2/3 of the ear canal lining. The numbers following the horizontal bars in Figure 2 relate to the references at the end of this post (numbers in parenthesis). The isthmus here, is described as between the first and second bends of the ear canal.
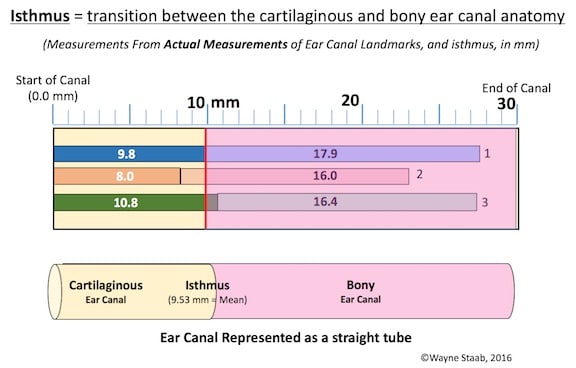
Figure 2. Location of the isthmus, based on actual measurements. The isthmus is described as being between the first and second bends of the ear canal, and is often the narrowest part of the ear canal.
Another way to look at the cartilaginous and bony ear canal is based on looking carefully at the ear impressions to determine where there are no skin pore markings completely around the ear canal8,9. The area of no skin pores (shiny impression surface) is thought to represent bony structure because there is no subcutaneous structure allowing sebaceous or ceruminous glands and/or hair follicles to show. This may be a suggested way to estimate 100% bony surrounding, but provides little or no useful information about the remainder of the cartilaginous and bony structure relationships. Additionally, checking for smoothness requires very high quality and low viscosity impression material, and is highly dependent on subjective judgments. An ear impression material used by this author to see these differences well is a 20 or 25-Shore Dur-A-Sil (formerly ReBound, and available from a number of sources). Most ear impression material will not allow one to see these differences. And, of course, the ear impression has to have sufficient length to be able to compare sections. A study reporting on making decisions about whether a section is underlined by bone or cartilage, based on this differentiation, suggests that the procedure is not easily performed since only 84 (9%) of 915 ear impressions were able to be evaluated using this procedure8. When applied, that portion of the ear canal reported to be completely surrounded (100%) by bone averaged 1.81 mm medially from the second bend8, meaning that a significant area proximal to and beyond the second bend continues to have substantial bone, even if less than 100%. Similar observations by this author reveal that much of the area around the second bend, and even into the isthmus, is lined by bone, at least partially.
The bony anatomy of the skull (specifically the temporal bone) provides some useful information about the bony canal. While the canal is fully encased in bone closer to the tympanic membrane, a bony shelf can extend well into the isthmus area in adults, as can be seen in the inferior portion of the ear canal (Figure 3).
Parasagittal plane computed tomographic (CT) images (0.6 to 1 mm slice thicknesses) were evaluated on 62 ears of individuals older than 18 years of age. Measuring from the annulus outward, OEAC (Osseous External Auditory Canal), results showed mean complete enclosure by bone of 9.8 mm, with a range from 4 to 17.4 mm for individuals older than 18 years of age11.
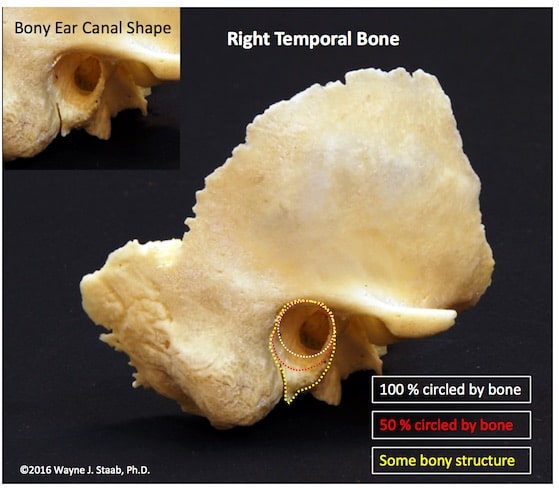
Figure 3. The bony shelf of the temporal bone extends well into, and past the second bend in adult ear canals, possibly into the isthmus area. It is tempting for some to conclude that the cartilaginous canal extends from the aperture of the ear canal to the complete encasement in bone, it is just as logical to contend that the bony portion extends from the tympanic membrane to where there is no bony substructure, meaning possibly to the isthmus.
Next week’s post will continue this discussion, focusing on the ear canal length, the location of the first and second bends, and the isthmus.
References
- Krumenacker, S. Chapter 9, Ear Impression Preparation, in Hearing Aid Dispensing Training Manual, Plural Publishing, 2013.
- College of Audiologists and Speech-Language Pathologists of Ontario. Preferred practice guidelines for ear impressions, Approved, March 2005, Reformatted, April 2014. caslpo.com.
- British Society of Audiology, Recommended procedure taking an aural impression, Feb, 2013, Review Feb 2018 thebsa.org.
- Westone video. https://www.youtube.com/watch?v=KiqFiLIVrB8)
- Taylor, B., and Mueller, H.G. Fitting and Dispensing Hearing Aids. All About Style: Hearing Aids and Earmolds, p. 183, Plural Publishing, Chapter 7, 2011.
- https://www.customearprotection.co.uk/about/our-products/taking-an-ear-impression/.
- Staab, W.J. and Sjursen, W. (2000). A one-size disposable hearing aid, American Auditory Society, March, Scottsdale, AZ
- Nielson, C. and Darkner, Sune. The cartilage bone junction and its implication for deep canal hearing instrument fittings, The Hearing Journal, Vol. 64, Issue 3, pp 35-36, 40, 42, 2011.
- Oliveira RJ, Hoeker R: Ear canal anatomy and activity. Sem Hear 2003;24(4):265–275.
- Staab, W.J. (2014). The human ear canal V, hearinghealthmatters.org, July 7.
- Mahboubi H, Wu EC, Jahanbakhshi R, Coale K, Rothholtz VS, Zardouz S, and Djalilian HR. A novel method to determine standardized anatomic dimensions of the osseous external auditory canal. Otology & Neurotology, Retrieved on: 22 February 2016.
(1) Ahmad, I, Lee, W.C., and Binnington, J.D. 2000. External Auditory Canal Measurements Localization of the Isthmus. Oto-Rhino-Laryngologia, Nova. Vol. 10, #5, 283-186. Departments of Otolaryngology and Audiology, Russells Hall Hospital, Dudley, UK
(2) Anatomy of the Human Body. Henry Gray (Gray’s Anatomy). Published online, May 2000 by com; © 2000 Copyright Bartleby.com, Inc.
(3) Tsung-Hsiun Tu, Jen-Fane Yu, Ren-Hung Wang, Yen-sheng Chen. 2014. Anthropometry of External Auditory Canal by Non-contactable Measurement. Center for Measurement Standards, Industrial Technology Research Institute, Taiwan, and Taiouan Interdisciplinary Otolaryngology Laboratory, Chang Gung University, Taiwan. noise 2014, Melbourne Australia, 16-19, November.


