

 Changes to the ear canal occur resulting from the aging process. Additionally, there are issues that must be considered when placing auditory (or other) devices into the ear canal. This is the last in our series on the human ear canal.
Changes to the ear canal occur resulting from the aging process. Additionally, there are issues that must be considered when placing auditory (or other) devices into the ear canal. This is the last in our series on the human ear canal.
Ear Canal Physiology – General
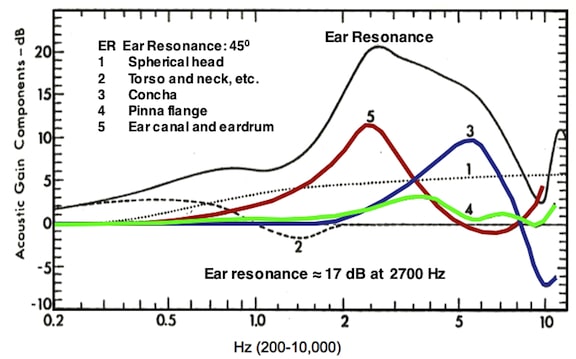
Figure 1. Components used in ear resonance. Ear resonance is the combination of the spherical head, torso and neck, concha, pinna flange, the ear canal, and the eardrum. Real-ear measurements place the ear resonance at approximately 17 dB and about 2700 Hz.
Previous posts have provided data showing the distance between the auricle (what we hook eyeglasses to) and the eardrum. The length of this distance is not accidental, and the following general features provide reasons for it.
- The ear canal distance (depth) helps protect the critical inner parts of the ear against trauma and temperature extremes.
- It serves as a channel between the ear mechanism and external environment.
- The ear canal acts as closed tube having a fixed length, resulting in a resonance of about 10 dB at about 2500 Hz (number 5 in Figure 1). However, when coupled with the gains provided by the pinna flange, concha, spherical head, torso and neck, it measures from about 15 to 20 dB at about 2700 Hz. Real-ear audiological measurements generally place the ear resonance at approximately 17 dB at about 2700 Hz.
- The two meati (canals) help localize sound sources, primarily from the front or back of head, to a limited extent.
General Comments About Canal Changes From Neonate to Adult
In the infant, the bony canal is very short prior to the development of the annulus and mastoid process. Also, the tympanic membrane is directed more inferiorly than laterally. There are essentially no data available on ear canal size for neonates, infants, or young children. It is thought that the ear canal is adult size by approximately the pre-teens.
Post-natal changes in the temporal bone (that are expected to have some impact on the overall size) are shown in Figure 2. From post-natal to adult, the temporal bone:
- Increases in size
- Changes the shape of the tympanic ring to form the cylindrical tympanic bone of the adult
- Deepens and changes in the direction of the face of the articular fossa
- Shows growth and pneumatization of the mastoid process (pneumatization not shown)
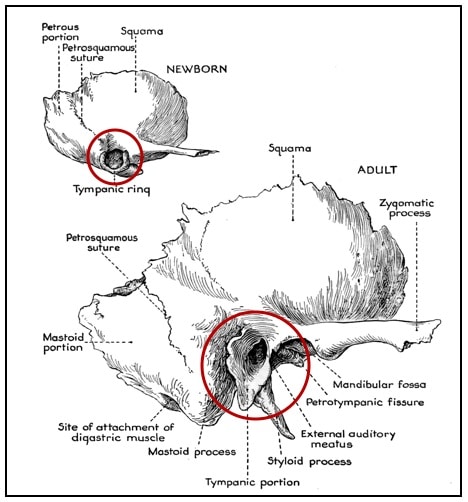
Figure 2. Changes in the human ear canal from neonate to adult. The areas circled in red reflect substantial changes in the osseous structure.
In a child up to the age of about 4 years, and sometimes in adults, the bony meatus is deficient anteroinferiorly. It is expected that the osseous meatus is complete by puberty state that the external auditory canal continues to develop until the seventh and maybe until the ninth year. Regardless, at birth the floor has no bony portion. In the infant, the EAM (external auditory meatus/canal) is short and straight, while in the adult the canal is longer and curves. The infant TM (tympanic membrane) is in an oblique or almost horizontal position, and is difficult to visualize.
Older Adult Ear Canal Changes
Changes specific to the ear canal indicate that the volume does not change with age (recall that the volume of the male ear canal is larger than that of females, in general). However, some changes lead to potential medical problems, and impact listening devices intended to be inserted into the ear canal. These include:
- Thinning of the surface epithelium
- Atrophy of the subcutaneous tissue
- Glandular structures of the ear canal lose some of their secretory abilities, resulting in skin that is dry, attenuated, and prone to trauma and breakdown
- Cerumen becomes more concentrated and is often hard and impacted. It has been suggested that 25% to 65% of patients admitted to skilled nursing facilities/nursing homes over the age of 65 have cerumen impaction that may affect hearing.
- Hair in males often becomes wiry.
- Collapsed canals
Other (Risk) Issues Related to Placement of Objects in the Ear Canal
The magnitude, severity, and significance of risk vary with each of these issues.
Cough reflex. This occurs with some individuals when objects are inserted into the ear canal. It is initiated by approximation to Arnold’ branch of the 10th cranial nerve (Vagus), which is located in the inferior-posterior ear canal. Manipulation of an object in that area provides for accommodation by most individuals.
Cerumen. Popularly known as ear wax, cerumen is a mixture of the secretions of two glands in the cartilaginous ear canal. One type of secretion comes from the large and active sebaceous glands that are associated with the hair follicles that secrete sebum; it is an oily mixture of fats, cholesterol, protein, and inorganic salts. Sebum is thought to have very mild anti-bacterial and anti-fungal properties. The other secretion comes from the ceruminous glands. These are essentially the same as the apocrine sweat glands of the armpit. The resulting mixture is a highly viscous, chemically complex, acidic combination of fats and waxes that coats the surface of the ear canal. The general composition of this combination of secretions is a variety of lipids, with trace amounts of mineral ions and amino acids. Mixed into this chemical brew are dust, dirt, bacteria, and discarded hair and skin cells.
Cerumen provides a chemical barrier that prevents infection of the canal, as well as providing a mechanical barrier that lubricates and protects the skin, prevents contact with water, bacteria, and other foreign objects, and carries debris away from the eardrum. Physiological action gradually pushes the wax and foreign substances trapped in it from the canal. The presence of a hearing aid or earmold in the ear blocks this natural process and can lead to an accumulation of debris in the canal.
The amount and specific composition of cerumen varies between races and individuals in each race. Caucasian and African individuals tend to have wet wax, which is moist, sticky, and golden-brown. Asians and Native Americans tend to have a wax that is dry, flaky, and more grayish in color.
In some individuals, the secreted cerumen tends to dry out and cake; in others, it remains the consistency of butter. Some are high secretors, and cerumen may build up again rapidly following removal. This may become worse in tropical climates or under conditions of bodily stress. This natural secretory function may also be stimulated in first-time users of hearing aids, as the ear tries to flush the “foreign object” from the canal. Conversely, some individuals are under-secretors, a condition that results in dry skin in the canal that itches and scales. Age and gender do not seem to be significant factors in cerumen production, although some older individuals tend to have drier wax due to general atrophy of the apocrine glands with age.
Some older men may have unusually dense hair growth in the ear that combines with wax and debris to form a plug that prevents emigrating cerumen from leaving the canal.
Conditions related to moisture/humidity. The build-up of heat in an ear canal occluded by a hearing aid or earmold, for example, also causes wax to vaporize within the ear canal. For an object that remains in the ear canal for numerous days, it may condense on any cooler object that it encounters, such as the speaker/receiver of a hearing aid placed in the ear canal. However, this may take at least six months before it has any significant impact.
Temperature in the ear canal (inside a hearing aid shell) is between 80 and 99 degrees F. Relative humidity is typically between 30% and 49% (also in a hearing aid shell). Indoor measurements are concentrated around 68 to 75 degrees F. Although temperature change (13 to 94 degrees F) seems to make little difference, there is a general increase in the humidity inside a hearing aid shell as the ambient humidity increases. Two opposing effects determine the deviation of the hearing aid relative humidity from ambient. Body temperature is generally higher than ambient temperature and this tends to decrease the relative humidity in the hearing aid; however, perspiration increases the relative humidity in the hearing aid.
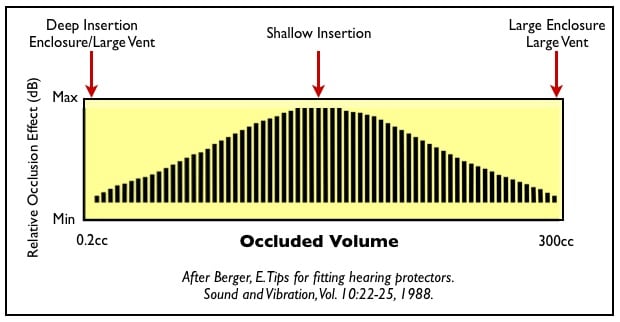
Figure 3. The magnitude of the occlusion effect (OE) is dependent upon the location of a device inserted into the ear canal, and on the opening, or access to large air volume.
Occlusion effect. The occlusion effect is a subjective increase in self-generated sounds when an ear canal is occluded, especially with a seal in the cartilaginous canal, and if a vent that allows sound to escape does not exist (at least 2 mm in diameter). This is most noticeable when the person talks or chews. The occlusion effect provides an undesirable listening experience and should be avoided (distortion, own voice is booming, masking of external acoustic signals, decreased word recognition). Figure 3 illustrates changes in the magnitude of the occlusion effect when measured with different volumes and reflecting
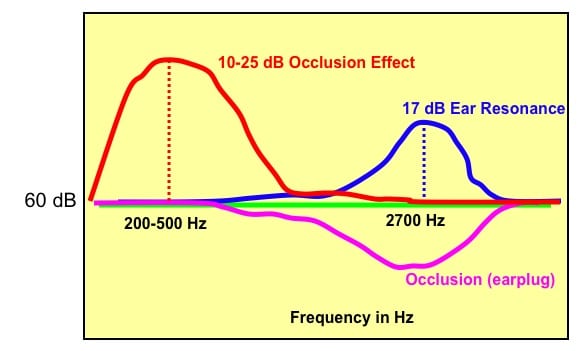
Figure 4. The occlusion effect (OE) is a low-frequency amplification of self-generated sounds under certain conditions, whereas occlusion is an attenuation or reduction of incoming sounds – the magnitude dependent upon how well the ear device acts as an earplug. Ear resonance is a high-frequency effect associated with an open ear canal, and is most often reduced by a device inserted into the ear canal. The greater the device acts as an earplug effect, the less the ear resonance. It is generally reduced completely, as shown by the earplug occlusion. Amplification is required to overcome this, but not in a linear application. If the occlusion reduction is 15 dB, it does not take 15 + 17 dB (32 dB gain) to overcome this. This is a parallel action related to amplification, not a linear, or serial action.
different coupling. Sealed coupling, when making contact more deeply into the osseous canal, essentially has no occlusion effect.
This illustration shows also that a shallow insertion of an earpiece into the ear canal (with no large vent) creates the maximum occlusion effect. The occlusion effect (OE) is not to be confused with occlusion, which is the result of closure of the ear canal leading to an attenuation of external sound sources. Stick your finger into your ear canal and listen. This is occlusion. Then phonate the long “e” sound (with finger inserted), and you will hear the increased loudness, or the occlusion effect.
Figure 4 illustrates the differences between measurements of the occlusion effect (OE), occlusion, and the ear resonance. Note that the OE and occlusion impact different parts of the auditory spectrum. The occlusion magnitude (attenuation) depends on how well the earpiece acts as an earplug.
Hearing Loss. It has been pointed out that the unoccluded ear acts as a resonator, generating approximately 17 dB of increased sound pressure at approximately 2700 Hz (Figure 1). When the ear canal is occluded, this “natural” amplifier is lost, and in fact, the blockage causes a further loss of hearing sensitivity, especially in the high frequencies (occlusion/attenuation). However, if a vent of at least 2 mm is present in the object placed in the ear canal, a hearing loss does not occur because of the blockage. Still, one might get a sensation that the ear is blocked, or partially blocked.
Trauma. Careless placement of an object in the ear canal can cause the skin, especially of the bony canal, to break or swell (in the form of an edema or hematoma). This is more likely to occur with a tightly fitting earpiece or for an object that is sharp and hard.
Collapsed canals. As individuals age, ear canals tend to collapse, thus reducing the size of the opening. This collapse occurs in the cartilaginous canal. The canal may open easily when an object is inserted.
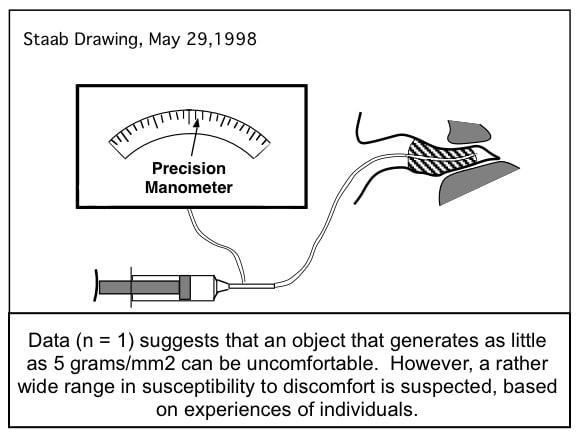
Figure 5. The osseous ear canal is highly sensitive to touch as recorded on this single subject, but confirmed via hundreds of subject interactions. It does appear, however, that subjects are able to find their sensitivity reduced follow a succession of insertions into that same region, and with successively longer wearing schedules.
Comfort. An object that fits more deeply in the ear canal, and having full contact, is more prone to discomfort. Data (n = 1) suggests that an object that generates as little as 5 grams/mm2 can be uncomfortable. However, a rather wide range in susceptibility to discomfort is suspected, based on experiences of individuals (Figure 5).
Security of fit. The bends of the ear canal help to hold an object in the ear canal, providing that the object has lines that are similar to the ear canal. Excessive mandibular movement can force an object from the ear canal under certain conditions (Figure 6). The mandibular action normally moves anteriorly during speaking or mastication, and then returns to its rest position. The action is to enlarge the ear canal in the area of the 2nd turn. This, in turn, can cause an object located in the ear canal, but not having good retention, to slip from the ear canal as the mandible returns to its rest position. It can also break the acoustic seal.
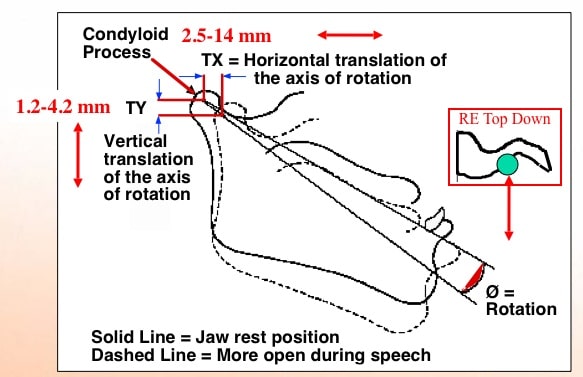
Figure 6. These measurements were made using cinefluorography (moving x-rays). This shows that the mandible moves in three translations: horizontal, vertical, and rotational.
Cosmetics. For hearing aids, cosmetics are often a primary issue with patients. For objects that are not hearing aids, this may be less of an issue, but it seems never to be eliminated as an issue.
Insertion. Because of the turns of the ear canal, the more closely an object to be inserted in the canal must fit, the more difficult is the insertion. An object can usually be inserted in the ear canal by a third party more easily. However, if the object does not have to confirm exactly to the ear canal turns, it also can be inserted more easily by the patient.
References:
- Mawson, S.R. 1967. Diseases of the Ear, Second Edition. Edward Arnold (Publishers) Ltd
- Northern, J. and Downs, M. Hearing in Children. 1975. The Williams & Wilkins Co., Baltimore
- John, AF and Santos-Sacchi, J. 1988. Physiology of the Ear. Raven Press, New York
- Agnew, J. 1994. Towards a better understanding of cerumen. The Hearing Review, April, 1994
- Bailey, J.W., and Valente, M. 1996. Measurements of relative humidity and temperature in hearing aids. The Hearing Journal, Vol. 49, No. 10, pp 59-63
Wayne Staab, PhD, is an internationally recognized authority in hearing aids. As President of Dr. Wayne J. Staab and Associates, he is engaged in consulting, research, development, manufacturing, education, and marketing projects related to hearing. His professional career has included University teaching, hearing clinic work, hearing aid company management and sales, and extensive work with engineering in developing and bringing new technology and products to the discipline of hearing. This varied background allows him to couple manufacturing and business with the science of acoustics to bring innovative developments and insights to our discipline. Dr. Staab has authored numerous books, chapters, and articles related to hearing aids and their fitting, and is an internationally-requested presenter. He is a past President and past Executive Director of the American Auditory Society and a retired Fellow of the International Collegium of Rehabilitative Audiology.
**this piece has been updated for clarity. It originally published on July 28, 2014


