
 It’s been two years since I discussed the skull vibration induced nystagmus test (SVINT) in the post Skull Vibration Induced Nystagmus Test: shaking up vestibular assessment?. Since that time, we have implemented skull vibration as a part of our regular vestibular assessment protocol.
It’s been two years since I discussed the skull vibration induced nystagmus test (SVINT) in the post Skull Vibration Induced Nystagmus Test: shaking up vestibular assessment?. Since that time, we have implemented skull vibration as a part of our regular vestibular assessment protocol.
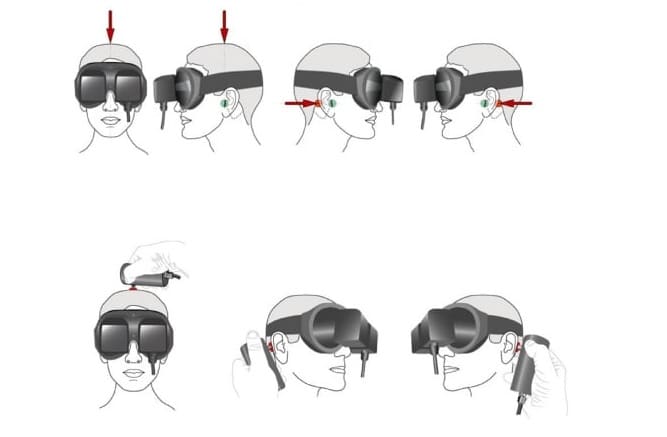
We currently utilize the North Coast Medical NC 70209 vibrator that is mentioned in the article The Skull vibration-induced Nystagmus Test of vestibular Function—A Review. This unit is a much cheaper alternative to the Bruel & Kjaer Minishaker 4810 utilized in some clinics. The North Coast medical vibrator is around $20 making it economically feasible.
The only other requirement is a set of video goggles that reduce visual suppression, which many clinics already have for completion of videonystagmogarphy (VNG) testing.
Our Clinical Observations
Unilateral Vestibular Loss
We find that clinicians are more likely to measure skull vibration induced nystagmus with greater degrees of unilateral peripheral vestibular hypofunction regardless of one’s central compensation status. Most often if a patient’s caloric examination shows a > 50 % caloric hypofuction, then a clinician is very likely to evoke skull vibration induced nystagmus. We have, however, seen skull vibration elicit nystagmus in patients with as little as a 30 % caloric hypofunction. It is important to note that calorics examine the vestibular ocular reflex (VOR) at an extremely low frequency while skull vibration examines the VOR at a high frequency and the two may not always correlate with one another.
We have also been able to evoke horizontal nystagmus by skull vibration in several patients with isolated unilateral otolith (saccule or utricle) dysfunction. Measures of horizontal semicircular canal function including calorics and the lateral video head impulse test (vHIT) were normal in both patients. Without skull vibration and vestibular evoked myogenic potentials (VEMPs), these two patients would have been told they had “normal” peripheral vestibular function.
Meniere’s Disease
In a Meniere’s disease population, we often see a pattern of normal vHIT and abnormal caloric irrigations. This is a pattern of vestibular test findings that are commonly found in a Meniere’s disease population. Skull vibration is a high frequency measure and will often best correlate with a high frequency measure such as vHIT, even if a patient has a significant caloric hypofunction.
If someone with Meniere’s recently experienced an episode of Meniere’s disease, we are more likely to generate skull vibration induced nystagmus. Also, if someone has spontaneous nystagmus associated with an episode of Meniere’s disease, skull vibration will most often increase the amplitude of the nystagmus. If a patient with Meniere’s disease has undergone any sort of ablative procedure such as gentamicin injections, then skull vibration is likely to be present at all times regardless of when the last episode of Meniere’s disease occurred. This is likely due to the more global labyrinthine deficit secondary to the gentamicin. Our findings are similar to reports in the literature on skull vibration testing.
Superior Semicircular Canal Dehiscence (SSCD)
This is the only patient population that we seem to have different observations than those mentioned in the The Skull vibration-induced Nystagmus Test of vestibular Function—A Review article. We have seen multiple patients with superior semicircular canal dehiscence (SSCD) that did not have skull vibration induced nystagmus with placement on the vertex or mastoids. These same patients went on to have abnormal ocular VEMP and cervical VEMP assessment consistent with SSCD.
It is possible this is related to our use of the NC Medical 70209 rather than the B&K Minishaker utilized in the majority of the peer-reviewed literature. At present, we cannot recommend skull vibration with the use of a NC Medical 70209 as being effective for detecting SSCD.
Central Etiologies
In our experience, it is extremely unlikely to elicit skull vibration induced nystagmus if a central cause is believed to be the sole contributor for one’s dizziness symptoms.
Summary
Overall, we have found skull vibration to be an effective, time efficient, comfortable way to assess vestibular patients and it is now an integral part of our test protocol. Our personal observations largely correlate to the findings in previous literature with the exception of superior semicircular canal dehiscence.
It is important to note that skull vibration is only part of our overall protocol, but it is a simple way to determine if a large degree of peripheral vestibular hypofunction exists regardless of one’s central vestibular compensation status.
Photo courtesy Science Direct


